Hirsutism
 DISORDERS ASSOCIATED WITH HIRSUTISM
DISORDERS ASSOCIATED WITH HIRSUTISM
Polycystic ovary syndrome (PCOS)
Familial hirsutism
Drug-induced hirsutism
Adrenal causes
Other associated disorders
Idiopathic hirsutism
Overview
Hirsutism is defined as the excessive growth of thick, dark hair in locations where hair growth in women is normally minimal or absent. Such male-pattern growth of terminal body hair usually occurs in androgen-stimulated locations, such as the face, chest, and areolae.
Although the terms hirsutism and hypertrichosis are often used interchangeably, hypertrichosis actually refers to excess hair (terminal or vellus) in areas that are not predominantly androgen dependent. Whether a given patient is hirsute is often difficult to judge because hair growth varies among individual women and across ethnic groups. What is considered hirsutism in one culture may be considered normal in another. For example, women from the Mediterranean region and Indian subcontinent have more facial and body hair than do women from Asia, sub-Saharan Africa, and Northern Europe. Dark-haired, darkly pigmented individuals of either sex tend to be more hirsute than blond or fair-skinned persons. In women, hirsutism exceeding culturally normal levels can be as distressing an emotional problem as the loss of scalp hair.
Basics
Hirsutism, by itself, is a benign condition primarily of cosmetic concern.
However, when hirsutism in women is accompanied by masculinizing signs or symptoms, particularly when these arise well after puberty, it may be a manifestation of a more serious underlying disorder, such as an ovarian or adrenal neoplasm. Fortunately, such disorders are rare.
Pathogenesis
Hirsutism can be caused by abnormally high androgen levels or by hair follicles that are more sensitive to normal androgen levels. Therefore, increased hair growth is often seen in patients with endocrine disorders characterized by hyperandrogenism, which may be caused by abnormalities of either the ovaries or the adrenal glands.
The physiologic mechanism proposed for androgenic activity consists of three stages: (a) production of androgens by the adrenals and ovaries, (b) androgen transport in the blood on carrier proteins (principally sex hormone–binding globulin [SHBG]), and (c) intracellular modification and binding to the androgen receptor.
In short, central overproduction of androgen, increased peripheral conversion of androgen, decreased metabolism, and enhanced receptor binding are each potential causes of hirsutism. For circulating testosterone to exert its stimulatory effects on the hair follicle, it first must be converted into its more potent follicle-active metabolite, dihydrotestosterone. The enzyme 5-α-reductase, which is found in the hair follicle, performs this conversion.
The severity of hirsutism does not correlate with the level of increased circulating androgens because of individual differences in androgen sensitivity of the hair follicles.
Testosterone stimulates growth, thereby increasing size and intensifying the pigmentation of hair. Estrogens act in an opposite manner by slowing growth and producing finer, lighter hairs. Progesterone has minimal effect on hair growth.
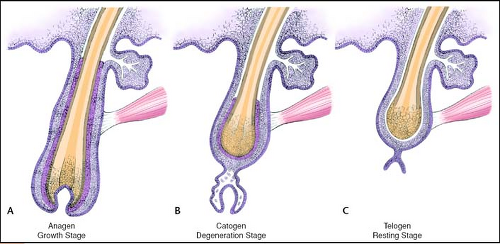 I11.1 Cycles of hair growth. (Modified from Structure and function of the skin. Sams WM Jr, Lynch PJ, eds. In: Principles and Practice of Dermatology. New York: Churchill Livingstone, 1990:8, with permission.) |
Cycles of Hair Growth
Hair grows in long cycles over many months: an anagen (active) phase (Ill. 11.1) is followed by a catagen (degenerative) phase, then a telogen (resting) phase, with different hairs alternating phases. The anagen and telogen phases are hormonally regulated. During the telogen phase, the hair shaft eventually separates from the follicle and falls out.
 11.1 Hirsutism. This patient has PCOS. This is the most common cause of androgen excess and hirsutism. Note the lesions of acne. |
The amount of free testosterone—the biologically active androgen that, after conversion to dihydrotestosterone, causes hair growth—is regulated by SHBG. Lower levels of SHBG increase the availability of free testosterone. SHBG decreases in response to the following:
Exogenous androgens
Certain disorders that affect androgen levels, such as polycystic ovary syndrome
Congenital or delayed-onset adrenal hyperplasia
Cushing’s syndrome
Obesity
Hyperinsulinemia
Hyperprolactinemia
Excess growth hormone
Hypothyroidism
Conversely, SHBG increases with higher estrogen levels, such as those that occur during oral contraceptive therapy. The resulting increased SHBG levels lower the activity of circulating testosterone.
Disorders Associated with Hirsutism
Polycystic Ovary Syndrome
The most common cause of androgen excess and hirsutism is polycystic ovary syndrome (PCOS).
Virilization is minimal, and hirsutism is often prominent.
Characteristic features include menstrual irregularities, dysmenorrhea, occasional glucose intolerance and hyperinsulinemia, and, often, obesity.
The hyperinsulinemia is believed to hyperstimulate the ovaries into producing excess androgens.
Women with PCOS may show other cutaneous manifestations of androgen excess in addition to hirsutism, such as recalcitrant acne (Fig. 11.1), acanthosis nigricans, and alopecia on the crown area of the scalp (a pattern that contrasts with the bitemporal and vertex androgenic alopecia seen in men) (see Fig. 10.2).
Hirsutism may also be seen in the following ovarian conditions, most of which are associated with virilization:
Luteoma of pregnancy
Arrhenoblastomas
Leydig cell tumors
Hilar cell tumors
Thecal cell tumors
 11.2 Familial hirsutism. As seen in this Pakistani woman, familial hirsutism is both typical and natural in certain populations. |
Familial Hirsutism
This type of hirsutism is not associated with androgen excess. Familial hirsutism is both typical and natural in certain populations, such as in some women of Mediterranean or Middle Eastern ancestry (Fig. 11.2).
Drug-Induced Hirsutism
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


