Abstract
Androgenic alopecia can be slowed and sometimes partially reversed with topical and medical treatments. However, the mainstay of correcting androgenic alopecia is with 1–4 hair follicular unit transplantation of follicles taken from the non-alopecic posterior scalp, harvested either through elliptical excision or follicular unit extraction. Robotic systems to automate follicular unit extraction are available. Patient expectations, continued progression of androgenic alopecia, as well as donor site hair density, quantity and quality are key considerations before having patients undergo hair transplantation. Medical treatment can help augment hair transplantation results. The role and effectiveness of low-level light therapy in the management of androgenic alopecia remains to be established. Men and women have different patterns of androgenic alopecia, but in properly selected patients both can undergo successful hair transplantation. Regeneration and cloning of hair follicles represent the next frontier in revolutionizing hair transplantation.
Keywords
hair transplant, hair transplantation, elliptical donor harvesting, follicular unit extraction, follicular grafts, robotic follicular unit extraction, androgenetic alopecia, male pattern hair loss, finasteride
Introduction
Hair frames our face and its length, color and style reflect our personality and how we perceive ourselves. The framing preserves a youthful facial appearance by shortening the face and returning the viewer’s focus to the center of the face. While hair is one of the few physical characteristics we can easily control, the inability to correct hair loss can lead to concerns regarding appearance and psychological stress. In the case of androgenetic alopecia, some individuals accept hair thinning as an unavoidable aging phenomenon, whereas others actively seek medical and/or surgical treatment options.
Historical Perspective
The first hair transplantation procedure for male pattern hair loss was successfully performed in the 1950s, using large punch autografts. Alternative techniques such as hair-bearing flaps and scalp reductions were also performed in an effort to redistribute hair or reduce the size of bald scalp. However, because of unsightly large “plugs”, obvious scars due to continued hair loss and an unnatural orientation of hair, these techniques were largely abandoned in favor of follicular unit grafts. The latter are placed into small “recipient” sites (0.5–1 mm in diameter) produced by a blade or needle. Follicular unit grafts can be obtained either manually or mechanically.
Male and Female Pattern Hair Loss (Androgenetic Alopecia)
Pathogenesis
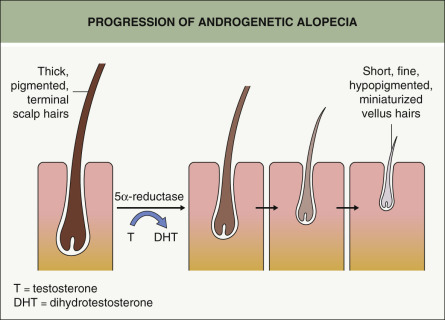
Miniaturization of terminal pigmented anagen hairs to fine hypopigmented vellus hairs is the hallmark of androgenetic alopecia (AGA; Fig. 157.1 ). Androgens, in particular testosterone and dihydrotestosterone (DHT), are required for the progressive reduction in hair follicle size with each cycle. The enzyme 5α-reductase, which is inhibited by drugs such as finasteride, converts testosterone to DHT (see Fig. 69.10 ). In addition to 5α-reductase isoenzymes (see Fig. 69.3 ), multiple androgen-metabolizing enzymes actually reside within the hair follicle itself, providing an explanation for “end-organ” sensitivity (see Fig. 69.4 ).
Stem cells, which reside in the hair follicle bulge, are responsible for hair follicle cycling and when these cells are destroyed, there is loss of the follicle. In mice, combining bulge cells with neonatal dermal cells can give rise to a hair follicle as well as the sebaceous gland and epidermis . Within the hair follicle, stem cells give rise to secondary germ cells with each hair cycle; the latter cells represent a progenitor population that is responsible for the production of the hair shaft during anagen (but undergoes apoptosis at the end of anagen) . In a study that compared bald scalp with hair-bearing scalp in men, the stem cell population was maintained in the bald scalp but there was a marked reduction in progenitor cells, suggesting that study of this second population of cells could provide further insight into male pattern hair loss .
In gene expression arrays, increased expression of the gene that encodes prostaglandin D2 synthetase was observed in bald scalp as compared to haired scalp in men with AGA ; the latter enzyme converts prostaglandin H2 (PGH2) to PGD2. Balding scalp was also found to have increased levels of PGD2, and PGD2 was shown to inhibit hair growth in explants of human hair follicles. This inhibition of hair growth by PGD2 required interactions with one of its receptors, pointing to a potential therapeutic target.
Population studies have pointed to a polygenic inheritance pattern, with both maternal and paternal genetic influences. Of the associated genes identified to date, the androgen receptor (AR) gene, present on the long arm of the X chromosome (Xq11–12), has been identified as a major determinant of hair loss in men . Within exon 1 of the AR gene is the AR-CAG polymorphism, which refers to the number of repeat sequences of cytosine–adenine–guanine (CAG) present, with the normal range of CAG repeats being 13–40. The number of CAG repeats appears to inversely correlate with the degree of androgen sensitivity. Men with fewer CAG repeats have an increased risk of developing AGA and a higher cellular sensitivity to androgens; they also demonstrate a greater response to finasteride treatment . In contrast, men with >40 repeats appear to be protected and have androgen insensitivity . Variants in the AR gene may influence hair loss in women as well .
The AR gene also has single nucleotide polymorphisms (rs6152; see Ch. 54 ) and Caucasian men with the A (adenine) allele have a low likelihood of developing AGA while those with the G (guanine) allele have a 70% lifetime risk of developing AGA, which increases to >80% if there is a positive paternal family history. Other implicated genes include EDA2R , which encodes the ectodysplasin A2 receptor and is also found on the X chromosome (see Ch. 63 ) , as well as genes located at 20p11 and 3q26 . As more insight is gained into the interplay of these genes, it may be possible to diagnose androgenetic alopecia at an early age and predict who may benefit from therapy. Of note, it is important for patients to realize that while a family history of androgenetic alopecia provides useful information, it does not predict the rate and extent of hair loss in a particular individual.
Clinical Features
The diagnosis of androgenetic alopecia is usually straightforward, especially in men. This is based upon the characteristic pattern, the miniaturization of hairs, and the lack of clinical inflammation (see Ch. 69 ). Occasionally, an unusual presentation requires clinicopathologic correlation, and if there is evidence of perifollicular erythema, the possibility of lichen planopilaris needs to be excluded . In women, patterned alopecia may first become clinically apparent as a result of a superimposed telogen effluvium, perhaps following a febrile illness or birth of a child. These patients require an evaluation for telogen effluvium as outlined in Table 69.3 and possible hyperandrogenemia (e.g. serum free testosterone, DHEA-S), especially in the setting of hirsutism and/or recalcitrant acne vulgaris or any signs of virilization. Female pattern hair loss has to be distinguished from other causes of alopecia, including central centrifugal cicatricial alopecia, early lichen planopilaris or frontal fibrosing alopecia, and diffuse alopecia areata; as a result, histologic evaluation may be required.
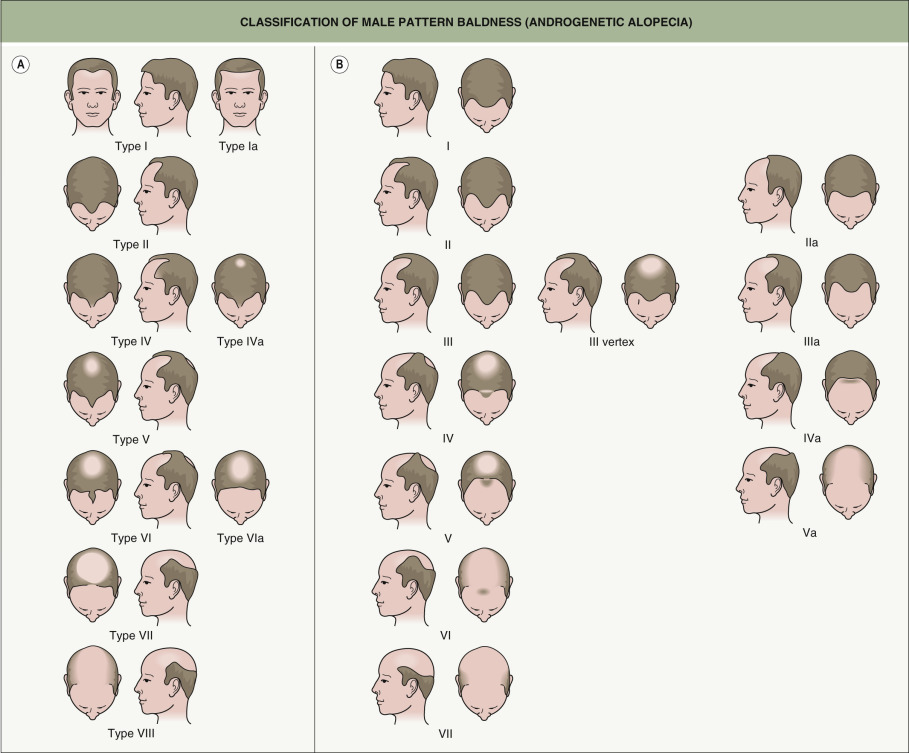
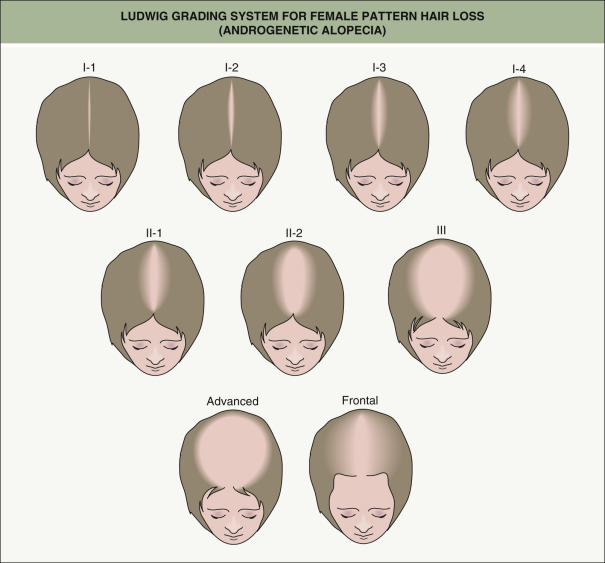
There are grading systems for androgenetic alopecia that allow assessment of severity, progression and response to therapy. In men, the Norwood classification ( Fig. 157.2 ) is used more often than the Hamilton classification system. Patterned hair loss in women is classically given a Ludwig grade (I, II or III; Fig. 157.3 ), even though the hair loss often has a Christmas tree pattern. Occasionally, the classification scheme for men is used.
Treatment (Other Than Transplant Surgery)
Medical therapies
Topical minoxidil as a 5% solution is FDA-approved for men whereas the 2% solution and 5% foam are approved for both women and men. In general, the therapeutic effects are modest, but it can prove helpful as an adjunct to hair transplantation . There is disagreement amongst transplant surgeons as to whether during the perioperative period topical minoxidil can stabilize existing hairs and shorten the time for transplanted hairs to grow. There is also ongoing debate with regard to minoxidil’s exact mechanism of action, but it is thought to be related to its vasodilatory or angiogenic properties and perhaps its effect on potassium channels . Increased proliferation of dermal papilla cells , an increase in hair caliber, a decrease in the rate of apoptosis of cells in the germinative pool, and more time spent in the anagen phase have all been observed .
A possible explanation for the variability in therapeutic responses amongst individuals is differing levels of sulfotransferase activity (which catalyzes minoxidil sulfate) in their hair follicles . Side effects of topical minoxidil include unwanted hypertrichosis of the cheeks or forehead, headache, ankle edema, and allergic or irritant contact dermatitis. With regard to the latter, propylene glycol in the vehicle is often the culprit and it has been removed from the 5% foam product (Rogaine ® ). The risk of facial hypertrichosis may be greater in those with a genetic propensity for dark facial hair. Fetal hypertrichosis has also been reported and so use of topical minoxidil is discouraged in pregnant or breastfeeding women.
Finasteride inhibits type II 5α-reductase, which converts testosterone to DHT and is present in hair follicles (see Figs 69.10 and 69.4 ). Oral finasteride (1 mg daily) is FDA-approved for men with AGA. In a randomized trial of 1553 men given either finasteride 1 mg or placebo for 1 year (with a blinded extension for a second year), significantly greater hair counts in the balding vertex were observed in those receiving finasteride . Five-year results from the same study demonstrated that hair growth peaked at 1–2 years, but hair counts still remained well above baseline for 90% of patients . Although finasteride was FDA-approved for stimulating the growth of vertex hairs, it also stimulates regrowth of frontal scalp hairs . Its use in combination with hair transplantation has yielded statistically greater hair counts 48 weeks after surgery in comparison to the control/placebo group . There is also some evidence that finasteride may work better in men with higher levels of DHT (such as those in their mid-twenties) .
Patients are advised to allow at least 6 months before expecting to see a therapeutic effect. If they discontinue the finasteride, the AGA will return to its pre-treatment appearance. Because finasteride is metabolized extensively in the liver, it should be used with caution in patients who have known liver disease . Finasteride also artificially lowers the serum prostate-specific antigen (PSA) level by ~50% . Therefore, both the primary care physician and the patient need to be made aware of this effect. Although early data from prostate cancer trials suggested that finasteride might increase the histologic grade (i.e. severity) of prostate cancer , subsequent analyses suggested a detection bias .
Overall, the drug is well tolerated. Side effects that occur in <2% of men taking finasteride include decreased libido, erectile dysfunction and ejaculation disorder, compared with their occurrence in 1% of the placebo group. Rarer side effects include gynecomastia, breast tenderness, and depression . In a double-blind, placebo-controlled, multicenter trial in young men, no changes in spermatogenesis or semen production were observed . However, there have been two reports of severe azoospermia leading to impaired fertility . While the authors feel comfortable prescribing finasteride for men who are planning to have children, it should be discontinued if there are fertility issues, before embarking upon more invasive infertility treatments. Lastly, there are reports of sexual dysfunction even after discontinuation of finasteride, sometimes referred to as post-finasteride syndrome, but the validity of this side effect has been questioned. Nonetheless, it should be discussed with the patient.
We encourage surgical candidates to stabilize their hair loss by taking finasteride for 6 to 12 months prior to hair transplantation. As stated previously, most men benefit from combination therapy ( Fig. 157.4 ). Patients who report sexual dysfunction side effects should discontinue the medication and, after an interval of 1–2 weeks, try every second- or third-day dosing.

Finasteride is not FDA-approved for women with AGA, and at a dosage of 1 mg daily, no improvement was observed in clinical trials . Of note, finasteride can cause feminization of the male fetus. In an uncontrolled series of normoandrogenic women, higher doses of 2.5 mg and 5 mg daily led to improvement in hair density in 62% and 81% of patients, respectively . If a decision is made to try higher-dose finasteride in a woman with female pattern hair loss, counseling regarding fetal risk and its off-label use is essential.
Dutasteride differs slightly from finasteride in that it blocks both the type I and type II 5α-reductase isoenzymes (see Fig. 69.3 ). It has been used off-label at a dosage of 0.5 mg daily for AGA in men who did not respond to finasteride, and increased hair counts were observed in a randomized, placebo-controlled trial . However, the drug’s half-life is 5 weeks, compared with 6–8 hours for finasteride. Thus, side effects are longer-lasting (several months) and more difficult to reverse. In a double-blind, placebo-controlled trial, men who received oral dutasteride (0.5 mg daily) versus placebo for 1 year had significant decreases from baseline in sperm count: by 28.6% at 26 weeks, 25% at 52 weeks, and 23% at 24 weeks after the trial ended . Sperm motility was also reduced at the latter time point. This potentially irreversible drop in sperm count and motility is an issue for men who still desire to have children.
Low-level light therapy
There has been emerging interest in the use of low-level light therapy (LLLT) for photo-biostimulation of hair growth. This was initially based upon the observation that laser hair removal can sometimes trigger paradoxical hair growth in the surrounding skin . Based upon their approval by the FDA as a medical device (rather than a drug), multiple LLLT products are commercially available. The patient combs light (650–700 nm) through the hair two to three times per week or wears a laser cap for a prescribed amount of time daily, with the expectation of hair growth. However, there have only been a limited number of published studies examining the effects of LLLT on hair growth . Skepticism remains as to whether LLLT can lead to clinically significant hair growth .
Hair Transplantation
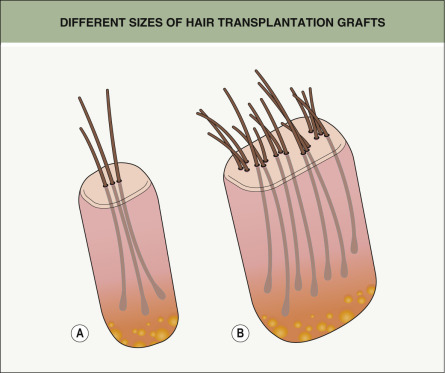
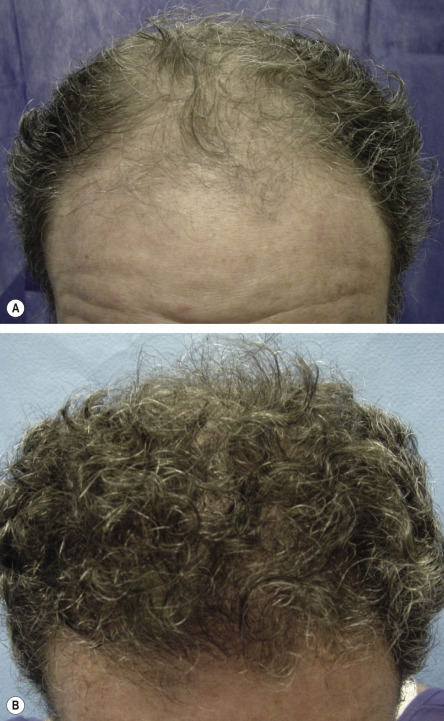
Hair transplantation is a procedure performed in an outpatient setting under local anesthesia. It is based on the theory of donor dominance, i.e. terminal hair from the unaffected posterior scalp will continue its growth pattern even when transplanted to the balding frontal scalp . Unfortunately, until the 1990s, hair transplants often had an unnatural appearance due to unsightly and obvious “plugs”, sometimes likened to a “Barbie-doll” appearance. Over the past two decades, there has been a revolutionary movement away from 3–4 mm grafts containing 15–30 hair follicles to grafts containing groupings of one to four hair follicles, referred to as individual follicular units ( Fig. 157.5 ). This has resulted in the transplanted hair having a more natural appearance ( Figs 157.6 & 157.7 ).

The net perceived density from a hair transplant is equal to the number of successfully transplanted follicles minus ongoing hair loss. In order to maximize long-term results, all patients undergoing this surgical procedure are encouraged to continue topical minoxidil and/or oral finasteride (see above). Halting or at least slowing the miniaturization process allows for the perception of greater hair density.
Candidate Selection
As with all surgical procedures, the preoperative consultation is key to the success of the procedure. The consultation establishes whether the patient is an appropriate or inappropriate candidate for hair transplantation, both from a medical and a psychological perspective. In addition, it allows for an assessment of areas of greatest concern and whether the patient has realistic expectations of what a hair transplant can achieve.
A complete medical, surgical and hair loss history is obtained, including previous hair transplants and scalp surgeries as well as scar formation. The etiology of the hair loss is determined, primarily via physical examination of the scalp. Occasionally, additional sites need to be examined and/or clinicopathologic correlation is required. The stage of patterned hair loss also needs to be established (see Figs 157.2 & 157.3 ). All medications, prescription, over-the-counter and herbal, are reviewed with regard to their effects on hair growth and hemostasis (see Chs 21 & 133 ).
The basic criteria for assessing the appropriateness of a candidate for hair transplantation are outlined in Table 157.1 . In particular, the density of donor hair in the occipital scalp and the caliber of the hair need to be appraised, as both have an impact on the perceived density of the transplant ( Table 157.2 ). Obviously, greater donor density and more grafts to transplant as well as thicker hairs rather than fine hairs lead to a fuller-appearing transplant.
| FIVE BASIC CRITERIA FOR ASSESSING CANDIDATES FOR HAIR TRANSPLANTATION | |
|---|---|
| Age | Patients over the age of 25 years are preferable. While patients younger than 25 years of age often seek consultation, there is a hesitancy to operate. The predictive value of future hair loss is much lower for individuals between 15 and 25 years of age. Even with the theoretical safety net of finasteride, physicians should carefully choose candidates under 25 years of age. This subgroup also tends to desire a return to a full head of hair as opposed to a mature pattern of restoration that is routinely performed in older age groups |
| Hair shaft caliber | The caliber of the hair shaft is crucial. Those with large-caliber hair shafts (greater than 70 microns) obtain much denser coverage than individuals with corn silk quality hair. This can be demonstrated mathematically in that very small volume increases in hair shaft diameter result in exponential increases in surface area coverage |
| Donor hair | A variety of instruments are available to measure donor hair density. Measuring a 0.25 cm 2 field and multiplying by four is the preferred method. Patients seeking hair transplantation who have >80 follicular units/cm 2 are excellent candidates. Those with donor hair density <40 follicular units/cm 2 are considered poor candidates |
| Degree of baldness | The degree of baldness is perhaps the most important criterion in candidate selection. Those with complete baldness of the frontal scalp as opposed to baldness limited to the vertex are excellent candidates. When frontal baldness is corrected, this creates the most dramatic positive change in appearance |
| Hair color | Follicular unit grafting has made hair color less of an issue than when punch grafts were employed. Color contrast between hair and skin can make grafts apparent if not transplanted with great care. Individuals with “salt-and-pepper” hair, red hair or blonde hair are preferential to those with jet-black hair. Black-haired individuals are not exempt as hair transplant candidates, but should receive only one-hair follicular units in the frontal hairline for the most natural result. Proper technique eliminates most problems with dark-haired candidates |
| HAIR TRANSPLANTATION – CLINICAL FINDINGS AND REALISTIC EXPECTATIONS | ||
|---|---|---|
| Clinical findings | Realistic expectations | Comment |
| 1000–1500 graft sessions will create the perception of increased hair density | Need to plan the procedure assuming the patient may stop the medication(s) and the hair loss will resume |
| 1000–1500 graft sessions may create little increase in perceived density | Although the transplant will result in more hair, this may not be apparent due to ongoing hair loss and thin-caliber hair |
Key Concepts
Both men and women should be made aware that AGA represents an ongoing process, i.e. it will progress despite undergoing hair transplantation. Medications (e.g. oral finasteride) can help to maximize hair density from a transplant by minimizing ongoing hair loss. However, in planning for the transplant procedure, the surgeon should always assume that in the future these medications may be discontinued (see Table 157.2 ). Also, the progressive nature of AGA means that additional hair transplants may be required, perhaps in another 5 or 10 years. The physician should therefore emphasize before the procedure how ongoing hair loss will affect the density and cosmetic appearance of the transplant as well as how this influences the placement of the grafts so as to assure a long-term natural appearance.
The number of expected procedures to accomplish both short- and long-term goals should be reviewed, as well as the limits on available donor hairs. Reasons for preferring to transplant primarily the frontal scalp as opposed to the vertex need to be explained – the vertex can consume donor grafts, it exhibits a continued 360° progression of hair loss which can lead to a peripheral rim of bald scalp, and this area of the scalp remains visible due to a central gravity pull. Concentrating the transplants in the frontal scalp will allow maximum long-term density with minimal long-term cosmetic risk.
Patients have to realize that elliptical donor harvesting will lead to a permanent scar of the posterior scalp ( Fig. 157.8 ). The scar is of no practical concern unless the patient has his or her hair closely cut. If the patient expresses an interest in having closely cropped hair, follicular unit extraction (FUE) should be considered (see below). However, the possibility of small “white dots” following FUE should be discussed. Lastly, the patient must appreciate the need for a conservative approach to placement of the anterior hairline so that it will have a natural appearance over a lifetime.










