Abstract
Free skin grafts are pieces of skin of variable thickness and size that are completely detached from their origin (donor site) to cover a defect (recipient site). Grafts for soft tissue reconstruction can be divided into four types: full-thickness skin grafts, split-thickness skin grafts, composite grafts, and free cartilage grafts. Knowledge of the indications, techniques, donor site considerations, and complications of all types of skin grafting is invaluable for the dermatologic surgeon who performs soft tissue reconstruction on a regular basis. With proper defect assessment, reconstructive planning, and attention to detail pre-, intra-, and postoperatively, optimal cosmetic and functional results using skin grafting techniques can be achieved.
Keywords
skin graft, full-thickness skin graft, split-thickness skin graft, composite graft, free cartilage graft, Burow’s graft, graft complications
- ▪
Free skin grafts are pieces of skin that have been severed from their local blood supply and transferred to another location
- ▪
Grafts for soft tissue reconstruction can be divided into four types: full-thickness skin grafts, split-thickness skin grafts, composite grafts, and free cartilage grafts
- ▪
In dermatologic surgery, grafts are most commonly used to repair defects created after removal of skin cancers; grafts also provide coverage and more rapid healing of leg ulcers
- ▪
The clinical situation determines the type of graft to be placed
- ▪
A working knowledge of the indications, techniques, donor site considerations, postoperative care, and postoperative complications of all types of skin grafting is essential for optimal soft tissue reconstruction
Introduction and Background
Skin grafting procedures originated approximately 2500 to 3000 years ago, when surgeons of the Hindu Tilemaker caste replaced noses amputated as punishment for theft and adultery with skin grafts harvested from the gluteal region . It was not until the nineteenth century, however, that skin grafting was reintroduced. In 1869, Reverdin’s account of pinch grafting for leg ulcers was published; in subsequent decades, Ollier and Thiersch’s accounts of thin split-thickness skin grafting, and Wolfe and Krause’s accounts of full-thickness skin grafting, appeared in the literature. While these and other nineteenth-century surgeons used skin grafts to address only the most difficult problems of surgical management, skin grafting has since evolved into a reconstructive option that is routinely, and sometimes preferentially, used for the surgical repair of skin defects.
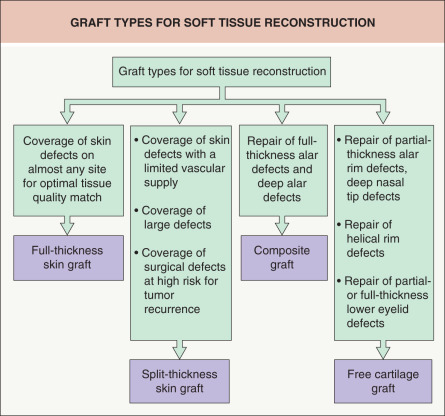
Free skin grafts are pieces of skin that have been severed from their blood supply and transferred to another location. They can be divided into four types: full-thickness skin grafts (FTSGs), split-thickness skin grafts (STSGs), composite grafts, and free cartilage grafts ( Fig. 148.1 ; Tables 148.1 & 148.2 ) . FTSGs are composed of the entire epidermis and the full thickness of dermis, including adnexal structures such as hair follicles and sweat glands. STSGs are composed of the full thickness of the epidermis and partial thickness of dermis. These can be subdivided into thin, medium and thick grafts, depending on the amount of dermis included in the graft. Composite grafts are composed of at least two different tissue types, usually skin and cartilage. Free cartilage grafts consist of cartilage with its overlying perichondrium.
| COMPARISON OF GRAFT TYPES USED IN SOFT TISSUE RECONSTRUCTION | ||||||||
|---|---|---|---|---|---|---|---|---|
| Graft type | Tissue match | Nutritional requirements | Requirement for recipient bed vascularity | Infection risk | Graft contraction risk | Durability | Sensation | Adnexal functions |
| FTSG | Good to excellent | High | High | Low | Low | Good to excellent | Good | Excellent |
| STSG | Poor to fair | Low | Low | Low | High | Fair to good | Fair | Poor |
| Composite | Good | High | Very high | Moderate | Low | Fair | Fair | Good |
| Free cartilage | NA | Moderate | High | Moderate | Migration or deformation possible, with subsequent resorption | Good | NA | NA |
| INDICATIONS, CONTRAINDICATIONS, ADVANTAGES AND DISADVANTAGES OF GRAFT TYPES USED IN SOFT TISSUE RECONSTRUCTION | ||||
|---|---|---|---|---|
| Graft type | Indications | Contraindications | Advantages | Disadvantages |
| Full-thickness skin graft (FTSG) | Coverage of skin defects, usually located on the face or scalp, requiring an optimal tissue quality match | Avascular graft bed | Excellent color and texture match Minimal graft contraction | Time consuming Donor site requires closure Requires meticulous technique |
| Split-thickness skin graft (STSG) | Coverage of large defects and defects with a limited vascular supply or at sites at high risk for tumor recurrence | Defects near free margins Facial defects in cosmetically sensitive areas | Increased chance of survival Ease of application Ability to cover large defects Able to act as a “window” to detect recurrence of high-risk tumors | Suboptimal cosmetic appearance Decreased durability Presence of granulating donor site wound Greater graft contraction Special equipment required to harvest larger grafts |
| Perichondrial cutaneous graft | Repair of deep nasal tip and alar defects, especially those with exposed cartilage | Avascular graft bed | Thicker than FTSG Contract less than FTSG Increased chance of survival under conditions of vascular compromise (compared to FTSG) | |
| Composite graft | Repair of full-thickness alar defects or nasal tip defects (<2 cm in diameter) with cartilage loss | Defects >2 cm in diameter | Single-stage procedure May yield good functional and aesthetic results when used to repair appropriately sized defects | Greater risk of graft failure under conditions of vascular compromise Graft size limitations (<2 cm) Limited donor tissue available Donor site may require flap or complex closure Increased risk of infection and graft displacement |
| Free cartilage graft | Repair of defects of nasal ala, tip or sidewall, ear or eyelid requiring restoration of structural support or preservation of contour of free margins | None | Provide structural support for selected facial and ear defects | Donor site may be painful Increased risk of postoperative infection Increased risk of graft displacement |
Wound Healing Considerations
Wound healing after skin grafting proceeds through a unique series of events . The first 24-hour period following graft placement is termed the stage of plasmatic imbibition, during which fibrin glue attaches the graft to its recipient bed, allowing it to take up the underlying wound exudate and to become edematous, gaining up to 40% in weight. The graft thereby remains hydrated and obtains a supply of nutrients, which maintains graft vessel patency until revascularization begins. The fibrin beneath the graft is subsequently replaced by granulation tissue, which attaches the graft permanently to its bed.
With proper apposition of the graft to its bed, revascularization may proceed. Anastomoses begin to form within 48–72 hours of grafting, between the recipient bed and pre-existing vessels in the dermis of the graft, a process known as inosculation. Vascular proliferation occurs next, with sprouting and budding of vessels in the graft and its bed. Even relatively avascular tissue may be grafted, as long as the avascular area is small and surrounded by a rich vascular supply. Through a process known as the bridging phenomenon, vascular connections arising from the recipient bed allow blood flow to occur through pre-existing graft vasculature, so that nutrients reach the part of the graft overlying the avascular area. Full circulation is restored to the graft within 4–7 days.
Restoration of the lymphatic circulation parallels restoration of the blood supply over the first week. Epidermal proliferation occurs between the 4th and 8th day post-transplant and persists for several weeks. Degeneration of sebaceous and eccrine glands may occur initially, but subsequent glandular regeneration may allow partial function to be maintained. Graft reinnervation and return of sensory nerve function may begin as early as 2–4 weeks after grafting, although patients do not usually regain full sensation for many months.
If extension of the ischemic period occurs, decreased graft survival may result ( Table 148.3 ). Hematoma or seroma formation, infection, or mechanical shear forces may disrupt the fragile vascular connections between the graft and its recipient bed. These complications tend to affect FTSGs (which have a greater volume to nourish and revitalize) more than STSGs.
| CAUSES OF GRAFT FAILURE | |
|---|---|
| Poor graft–bed contact | Hematoma |
| Seroma | |
| Shearing forces due to excessive postoperative activity | |
| Shearing forces due to inadequate immobilization of graft | |
| Poor recipient bed vascularity | Inadequate vascular bed (e.g. previous radiotherapy) |
| Exposed cartilage, bone, tendon | |
| Nicotine-induced vasoconstriction | |
| Infection | Coagulase-positive Staphylococcus spp. |
| Beta-hemolytic Streptococcus spp. | |
| Pseudomonas spp. | |
| Host factors | Diabetes mellitus |
| Immunosuppression | |
| Poor general health | |
| Nutritional deficiencies, including hypoalbuminemia | |
| Systemic conditions with vascular compromise | |
| Technique | Rough handling of tissue |
| Excessive devitalized tissue in recipient bed due to cautery | |
| Increased tension on graft due to inadequate size | |
| Inadequate hemostasis | |
| Inadequate trimming of adipose layer | |
| Placement of upside-down graft (more common with STSG) | |
| Inadequate anchoring (composite and free cartilage grafts) | |
Even after the ischemic period is past, other factors may combine to decrease the vascular supply nourishing the undersurface of the graft . The most important of these factors is cigarette smoking , but diabetes mellitus, protein deprivation, and severe trace element or vitamin deficiencies may also increase the risk of graft failure. Certain systemic medications, such as corticosteroids, chemotherapeutic agents, other immunosuppressive drugs and anticoagulants, may interfere with wound healing as well.
Other causes of graft failure include: insufficient vascularity due to necrotic debris within the recipient bed, hematoma, seroma, an avascular wound bed, previous radiotherapy, infection, excessive graft tension, mechanical shearing forces, and improper postoperative care (see Table 148.3 ) . The most common infectious agents associated with graft failure include coagulase-positive staphylococci, β-hemolytic streptococci, and Pseudomonas spp. Pseudomonal infections are particularly common in auricular grafts. For all of these reasons, a thorough preoperative evaluation, meticulous intraoperative technique, and good postoperative care are essential to maximize graft survival.
Full-Thickness Skin Grafts
Indications/Contraindications
FTSGs are most commonly used to repair facial defects resulting from the removal of skin cancers. They may be used to repair defects at virtually any site, as long as the recipient bed has both a sufficiently rich vascular supply to promote capillary regrowth and fibroblasts to supply collagen for graft adherence. Small avascular areas may be grafted due to the bridging phenomenon. Larger areas of avascular tissue, including patches of exposed bone, cartilage, tendon or nerve devoid of periosteum, perichondrium, peritenon or perineurium, respectively, are unable to support FTSGs. For this reason, FTSGs should not be placed over such avascular tissue.
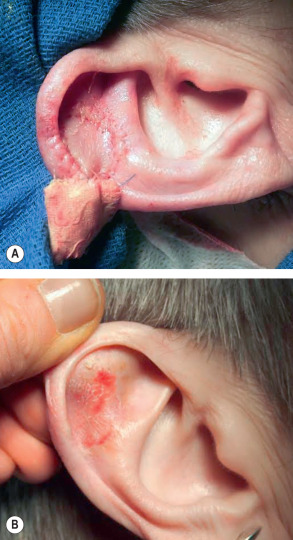
Under the proper circumstances, FTSGs can provide excellent color, texture, and thickness matches for facial defects because they include the full thickness of epidermis and dermis. Wound contraction is minimized since the full thickness of dermis is present, and dermal adnexal structures remain intact . FTSGs may be especially useful for the cosmetically and functionally acceptable repair of defects of the nasal tip, dorsum, ala and lateral sidewall, as well as the lower eyelid and ear ( Fig. 148.2 ) .
Preoperative History and Donor Site Considerations
A thorough preoperative evaluation that includes questions regarding bleeding tendencies, alcohol use, use of anticoagulant medications (including aspirin and nonsteroidal anti-inflammatory drugs), and a history of hypertension can help assess the risk of excessive bleeding and clot formation beneath the graft postoperatively . Diabetes mellitus, nutritional deficiencies, cigarette smoking, or the use of other nicotine-containing products may increase the risk of graft failure, and any history of these should be identified preoperatively.
Selection of a donor site for full-thickness skin grafting depends upon the color, texture, thickness, and sebaceous qualities of the skin surrounding the defect ( Tables 148.4 & 148.5 ). Most FTSGs are taken from sun-exposed areas above the shoulders whose color, vascular pattern, texture, and distribution of adnexal structures best match the skin surrounding facial defects. The thinnest grafts are usually harvested from the upper eyelid or the postauricular sulcus. Medium-thickness grafts are often harvested from the preauricular and cervical regions, while thicker grafts may be taken from the supraclavicular or clavicular region, conchal bowl, or nasolabial fold. Donor skin thickness, irrespective of site, will vary from one patient to another. It is therefore important to examine all sites carefully to find the best possible tissue match. This approach will ensure optimal donor site selection for each individual patient and surgical defect.
| DONOR SITE CONSIDERATIONS FOR FULL-THICKNESS SKIN GRAFTS | |
|---|---|
|
|
| SUMMARY OF POSSIBLE FULL-THICKNESS SKIN GRAFT DONOR SITES FOR DEFECTS IN DIFFERENT LOCATIONS | |
|---|---|
| Defect sites | Donor sites |
| Nasal dorsum, sidewalls, tip | Preauricular region, supraclavicular region or lateral neck (if large) |
| Nasal tip, ala | Preauricular region, conchal bowl, nasolabial fold |
| Junction of nasal dorsum/tip | Burow’s graft |
| Ear | Postauricular sulcus, preauricular cheek |
| Lower eyelid/medial canthus | Upper eyelid, postauricular sulcus |
| Scalp | Supraclavicular region, lateral neck, inner upper arm |
| Forehead | Burow’s graft, supraclavicular region, lateral neck, inner upper arm (if large) |
A regional approach may at times be used to obtain the best possible match for a given defect. Grafts taken from redundant upper eyelid skin may be used to repair lower eyelid defects, providing a good color and texture match in addition to a well-camouflaged donor site scar. Grafts used for lower eyelid defects should be oversized by 100–200% to allow for contraction and to avoid ectropion. Due to its relatively large size and inconspicuous location, postauricular skin may also be useful as a donor site for eyelid and auricular defects. Because postauricular skin is relatively non-sun-exposed, grafts harvested from this region may not provide a good color or texture match for other facial defects.
Preauricular skin is more versatile and can be used to repair most nasal defects, since the thickness and degree of sun exposure of these areas tend to be comparable. Donor site scars in this region can be easily camouflaged, as in facelift surgery, to provide a cosmetically desirable result. Even bearded individuals have a 1–2 cm hairless zone in the preauricular region. Care must be taken not to harvest hair-bearing skin in grafts taken from this area. Accidentally including mature follicular units may produce undesirable hair growth within the graft. Hair-bearing skin from the temporoparietal region may be used to repair eyebrow defects, where survival of the follicular units after transplantation may help to produce a superior cosmetic result. Skin from the nasolabial fold or the conchal bowl can sometimes be used to graft small nasal tip defects . At times, sufficient skin laxity may be present, particularly on the nose or forehead, to allow for partial defect closure by utilizing the adjacent Burow’s triangle as a FTSG, providing an excellent tissue match .
For larger defects requiring FTSGs of sun-damaged skin, such as the forehead and scalp vertex, the supraclavicular region or lateral neck can be used as a donor site. Again, care must be taken not to harvest unwanted hair along with the graft. These donor sites are often more difficult to camouflage, and must be carefully placed, especially in areas that might not always be covered by clothing. Although the color and texture match may be suboptimal, areas below the neck with thin, redundant skin, such as the upper inner arms, forearms and inguinal area, can be used.
Description of Technique
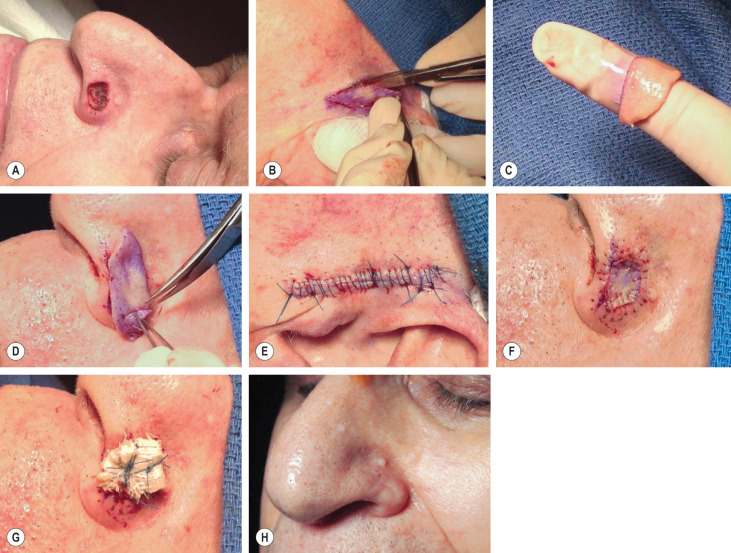
Varying techniques for harvesting and placing FTSGs have been described . To perform a FTSG, a template of the defect is first made, using any flexible material, such as gauze, Telfa™ or aluminum foil, which can be bent to conform to the defect ( Fig. 148.3A ). After marking the periphery of the recipient site with a marking pen, the template material is pressed against the defect, and the resulting outline of the inked margin serves as a guide to cut a perfect template. The template is applied to the donor site, and inking material is applied around it ( Fig. 148.3B ). The graft should be 3–5% larger in size than the true template to allow for the natural contraction and shrinkage of the graft after it has been harvested. Often, just cutting around the outside of the inked margin accounts for this extra “safety” skin. For eyelid defects, grafts should be oversized significantly, to minimize the risk of ectropion. Marking the donor site prior to local anesthesia prevents incorrect sizing due to tissue stretch from lidocaine infiltration. It is important to note that a donor site ellipse with a 3 : 1 ratio may not always be required, allowing for smaller donor site defects .
After the donor site is marked, local anesthesia may be injected into the donor and recipient sites. Epinephrine (adrenaline) may be used without compromising graft survival. If waterproof ink is not available for template marking, the outline of the template may be scored on the donor site with a needle. The donor site and recipient beds are then scrubbed with an antibacterial preparation such as chlorhexidine, rinsed with saline, and draped with sterile towels.
The donor site is excised with a scalpel to the level of the subcutaneous fat ( ![]() ). The graft is placed in a sterile bowl or Petri dish containing sterile normal saline, where it may remain for up to 1–2 hours. Grafts may be utilized up to 24 hours after harvesting if refrigerated or kept on ice. Before suturing the graft into place, defatting should occur. This is an essential step, since direct contact between the graft and its bed allows for connections between existing vessels as well as new vessel growth and nutritional support from the base of the defect. Adipose tissue adherent to the graft is poorly vascularized and is therefore not a good medium for new vessel growth between the graft and its bed.
). The graft is placed in a sterile bowl or Petri dish containing sterile normal saline, where it may remain for up to 1–2 hours. Grafts may be utilized up to 24 hours after harvesting if refrigerated or kept on ice. Before suturing the graft into place, defatting should occur. This is an essential step, since direct contact between the graft and its bed allows for connections between existing vessels as well as new vessel growth and nutritional support from the base of the defect. Adipose tissue adherent to the graft is poorly vascularized and is therefore not a good medium for new vessel growth between the graft and its bed.
When defatting is performed, the graft is placed dermal-side-up on the fingers or in the palm. All fat is trimmed from the underside using sharp scissors ( ![]() ). Fat is adequately removed when all of the yellow globular material is gone, leaving a white glistening dermal surface ( Fig. 148.3C ,
). Fat is adequately removed when all of the yellow globular material is gone, leaving a white glistening dermal surface ( Fig. 148.3C , ![]() ). If indicated, part of the dermis can also be trimmed to allow for differences in recipient site depth, although adnexal structures may be removed in the process, potentially altering the cosmetic result. The graft is then placed dermis-down in its bed, and rotated and trimmed if necessary, to achieve a perfect fit ( Fig. 148.3D ,
). If indicated, part of the dermis can also be trimmed to allow for differences in recipient site depth, although adnexal structures may be removed in the process, potentially altering the cosmetic result. The graft is then placed dermis-down in its bed, and rotated and trimmed if necessary, to achieve a perfect fit ( Fig. 148.3D , ![]() ,
, ![]() ). While one surgeon is trimming the graft, another may close the donor site, usually in a linear layered fashion with bilateral removal of standing cones ( Fig. 148.3E ). If the conchal bowl is the donor site, a 2 or 3 mm punch biopsy instrument may be used to remove full-thickness discs of cartilage from its central aspect, thereby facilitating second intention healing from the underlying dermis.
). While one surgeon is trimming the graft, another may close the donor site, usually in a linear layered fashion with bilateral removal of standing cones ( Fig. 148.3E ). If the conchal bowl is the donor site, a 2 or 3 mm punch biopsy instrument may be used to remove full-thickness discs of cartilage from its central aspect, thereby facilitating second intention healing from the underlying dermis.
Contouring of donor skin in FTSGs may be challenging, particularly when repairing defects on the nasal tip, ala, lateral nasal sidewall, helical rim of the ear, and eyelid . Graft contouring often requires multiple trial placements within the recipient bed, as well as multiple trimmings, to obtain an optimal result. Removal of cartilage not needed for structural support may increase the chance of graft survival, particularly for auricular defects, without compromising the aesthetic appearance of the repair .
Securing the Graft
Perimeter sutures, basting sutures, support dressings, or a combination of any or all of these can be used to anchor the FTSG. Depending upon the graft’s size, four to eight interrupted 5-0 or 6-0 absorbable or non-absorbable sutures may be placed at opposite edges of the graft periphery (e.g. at 3, 6, 9 and 12 o’clock) to tack down its four quadrants. A simple running suture, such as 6-0 fast-absorbing chromic gut suture, may then be placed around the graft’s perimeter ( Fig. 148.3F , ![]() ). Great care is taken to achieve perfect epidermal wound approximation. The running suture is placed in almost epicuticular fashion, passing the needle first through the graft and then through the surrounding skin. Placing the suture slightly higher in the dermis on the graft side and slightly deeper in the dermis of the surrounding skin makes suture placement easier, prevents tenting of the graft edges, and maximizes graft–recipient bed contact.
). Great care is taken to achieve perfect epidermal wound approximation. The running suture is placed in almost epicuticular fashion, passing the needle first through the graft and then through the surrounding skin. Placing the suture slightly higher in the dermis on the graft side and slightly deeper in the dermis of the surrounding skin makes suture placement easier, prevents tenting of the graft edges, and maximizes graft–recipient bed contact.
The use of tissue adhesives in full-thickness skin grafting has been investigated. In an initial pilot study, it was found that using cyanoacrylate tissue adhesive to secure FTSGs to their recipient bed wound edges produced cosmetic results essentially identical to those achieved with suturing . Because these adhesives set virtually instantaneously, the graft must be perfectly trimmed and aligned before adhesive application, since fine adjustments in positioning the edges of the graft are not easily made. Tissue adhesives may represent a useful time-saving alternative for securing the periphery of certain grafts, particularly those in relatively immobile areas such as the temple, forehead, and distal nose.
Basting sutures, usually simple interrupted 6-0 fast-absorbing gut sutures, can occasionally be placed to secure the central portion of the graft. They can be useful in securing large grafts to provide extra support against movement, as well as grafts placed on a concave surface where tenting could possibly occur. All sutures should be snug, but not strangulating, so as to not compromise graft survival.
Immobilization of the graft over its bed can be maximized with pressure dressings. Classically, tie-over bolster dressings have been employed to immobilize grafts, using anchoring stents to ensure direct contact between the graft and its bed . These stents may consist of various materials such as Xeroform™ gauze (bismuth tribromophenate-petrolatum-impregnated gauze), cotton balls, foam rubber, sponges, plastic beads, or disks . Although sutures or skin staples are usually employed to anchor the stent, adhesive wound closure tapes or Steri-Strips™ can also be applied to exert even pressure on the bolster . Adherence of the dressing to the graft, which tends to pull the graft from its bed at the time of dressing removal, is minimized by first applying petrolatum ointment, a non-adherent contact dressing, or Xeroform™ gauze to the graft site. Pressure or tie-over dressings help to immobilize the newly placed graft during the critical period of revascularization, and they help to prevent hematoma or seroma formation. Some authors postulate that such dressings may not be necessary to secure very small FTSGs .
The simplest bolster consists of Xeroform™ gauze alone, which is molded and placed to apply pressure to the graft ( ![]() ). One end of each of the peripheral non-absorbable sutures is cut long, to a length of approximately 3–6 cm, and its opposing suture is left uncut. The suture ends can then be tied over the dressing two at a time (i.e. 12 o’clock to 6 o’clock and 3 o’clock to 9 o’clock) to secure the bolster ( Fig. 148.3G ,
). One end of each of the peripheral non-absorbable sutures is cut long, to a length of approximately 3–6 cm, and its opposing suture is left uncut. The suture ends can then be tied over the dressing two at a time (i.e. 12 o’clock to 6 o’clock and 3 o’clock to 9 o’clock) to secure the bolster ( Fig. 148.3G , ![]() ). Alternatives to tie-over sutures include the running bolster suture, staples, and the “Lilliputian” technique . A light dressing consisting of Telfa™ and Hypafix ® may be placed over the graft. The donor site is dressed with a pressure dressing for 24 hours.
). Alternatives to tie-over sutures include the running bolster suture, staples, and the “Lilliputian” technique . A light dressing consisting of Telfa™ and Hypafix ® may be placed over the graft. The donor site is dressed with a pressure dressing for 24 hours.
Postoperative Care
After the pressure dressings are removed, careful wound care should be performed once to twice daily. One method is to gently clean both the donor site and the area immediately surrounding the bolster with hydrogen peroxide to remove all crusts, followed by application of petrolatum ointment (Vaseline ® ). The bolster is not disturbed until dressing removal at 1 week, at which point the bolster and all tie-over sutures are removed. Steri-Strips™ may be applied to the donor site as needed after suture removal.
The ideal graft is light pink when the bolster is removed. Its color may range, however, from pink or red to darker blue or purple, depending on the extent of graft revascularization. Patients should be cautioned about these color changes beforehand. A bluish tinge may be a sign of ecchymosis rather than graft failure. At this 1-week time point, a white graft is a sign that the graft has not revascularized and will fail, requiring the underlying wound to heal by second intention. A black graft signals necrosis and is undesirable. It is possible that the entire epidermal surface may become black and necrotic and then slough without adversely affecting the dermal portion of the graft, as re-epithelialization can occur from adnexal structures and the epithelial edges, with an acceptable cosmetic result. Therefore, eschars should not be debrided, since they can serve as natural dressings under which healing will progress. Patients should be counseled that the vascular supply of the graft remains fragile for weeks. For this reason, trauma, including direct shower water to the area, and excessive activity should be avoided for an additional 1 to 2 weeks.
When there is a good color and texture match between the FTSG and the surrounding skin, the cosmetic result is excellent ( Fig. 148.3H ).
Variations/Unusual Situations
Purse-string suture
The purse-string suture is a subcuticular stitch placed around the periphery of a circular or oval surgical defect . This type of suture allows partial defect closure by advancing skin from the entire periphery of the wound, and it may help to cover areas of exposed cartilage or bone at the wound edges that could inhibit graft take. In addition, the graft required to cover the remainder of the defect is greatly reduced in size due to an ~50% decrease in the defect area. Because of this reduced defect size, the graft needed to complete the repair may be harvested from traditional preauricular, postauricular or supraclavicular donor sites, which provide the best color, texture, and thickness match for most sun-exposed areas. Furthermore, FTSG placement decreases the risk of significant wound contraction, resulting in better cosmetic and functional results than would be produced by split-thickness skin grafting or second intention healing.
Large scalp defects extending to bone can present a significant management challenge, which can be handled by placing a purse-string suture followed by a galeal hinge flap . After purse-string placement, the galea aponeurotica adjacent to the scalp defect is scored with a scalpel, and a partial-thickness galeal flap of sufficient size to cover all or a portion of the exposed periosteum or bone may be dissected free and transposed into place, using the same motion as turning a page of a book. This hinged galeal tissue serves to recreate the vascular bed required for successful graft placement, and it permits repair of deep and often difficult scalp defects in a single operative session.
Burow’s grafts
Defects of the nasal sidewall and dorsum, and sometimes of the forehead, lateral neck or other areas, may be repaired with Burow’s grafts . Because Burow’s grafts utilize skin adjacent to the defect, they tend to provide a cosmetically superior match compared to grafts harvested from distant locations. These grafts are harvested from the skin superior to the defect if on the nose, and medial or lateral to the defect if on the forehead. The Burow’s triangle is excised (see Ch. 146 ) and the resulting donor defect is closed primarily, thereby partially decreasing the original defect size. The triangle is defatted, trimmed, and sutured into the defect. Operating time is decreased because a separate donor site is not required. Burow’s grafts tend to be limited in size. When insufficient laxity is present for partial donor site closure, or if the Burow’s triangle does not appear to be sufficiently large to cover the remaining defect, alternative donor sites should be sought.
Deep nasal defects
Deep postsurgical defects on the nose may at times pose a challenge for repair. Delaying FTSG placement for 12 to 14 days may increase the likelihood of graft survival over defects of the nasal tip and ala with denuded cartilage . Also, when tissue loss is deep in these areas, delaying skin grafting for 7 to 14 days may allow granulation tissue to fill in the defect such that a better contour may ultimately be achieved . Because the early granulating wound produces an excellent vascular bed, delayed grafting may be considered in patients with reduced wound bed vascularity, e.g. those who smoke or have had previous radiotherapy. At the time of delayed graft placement, the wound bed is debrided by rubbing with dry gauze and the edges are refreshed by scraping the wound edges with a scalpel held perpendicular to the edge. Prophylactic antibiotics are often prescribed when placing delayed grafts.
If a depressed defect is anticipated, but immediate reconstruction is preferred, dermal grafts can be used as a tissue filler prior to FTSG placement . Dermal grafts can effectively fill the defect, with little risk of resorption, and eliminate the need for a more complicated repair choice. The “drumhead” graft repair of deep nasal alar defects involves application of an overlying rigid plastic suspension coupled with an undersized graft, thereby preventing graft depression and nasal valve collapse; a cut portion of the periphery of the sterile plastic packaging from a suture packet can serve as the plastic suspension .
Perichondrial cutaneous grafts (PCCGs) are actually composite grafts composed of full-thickness skin and subjacent perichondrium; PCCGs may be used as a substitute for FTSGs when reconstructing deep nasal tip and alar defects, particularly those with exposed cartilage . PCCGs are harvested from the conchal bowl, utilizing the subperichondrial plane as the plane of dissection. The cartilage is not removed, making this graft more analogous to a FTSG than a cartilage-containing composite graft. The advantages of PCCGs over FTSGs include the following: PCCGs are thicker, have a greater chance of survival under conditions of vascular compromise, contract less than FTSGs, and may achieve better skin texture match on the distal nose due to the sebaceous nature of conchal bowl skin.
Postoperative Complications
The complications of full-thickness skin grafting can be divided into short-term problems of graft failure and long-term functional and cosmetic problems . Short-term problems include infection, hematoma, seroma, and shearing of the graft over its bed. These problems are significant when they occur, but can usually be avoided. Infection after grafting of facial defects, in particular, is not often encountered, and oral antibiotics are not routinely given postoperatively. Nevertheless, it is important to be gentle while handling tissue intraoperatively and to minimize devitalized tissue created by electrocoagulation in order to minimize the risk of infection. Prophylactic oral antibiotics covering Staphylococcus and Streptococcus spp. may be helpful in selected patients, especially those with diabetes mellitus, immunosuppression, or a prolonged intraoperative time. Grafts on the ears, fingers, and legs may benefit from prophylactic antibiotics, as these sites seem more prone to postoperative wound infections.
Hematoma and seroma formation can be avoided by meticulous hemostasis intraoperatively, pressure dressings, and postoperative caution. After consultation with the patient’s internist, cardiologist or primary care physician, patients may be instructed to avoid aspirin for 10 days before surgery, nonsteroidal anti-inflammatory drugs for 5 days before surgery, and alcohol for 2 days before and 2 days after surgery. In the past, patients taking antithrombotic medications were advised to discontinue these medications prior to surgery if their internist or cardiologist were in agreement. The current recommendations for management have, however, changed. While the risk of bleeding complications increases slightly if oral anticoagulants are not discontinued, most dermatologic surgeons do not routinely request that these medications be discontinued before surgery, since the risk of morbidity from hemorrhagic complications is minimal compared to that of the thrombotic events potentially associated with discontinuing these medications . Patients are also advised not to engage in vigorous activity, heavy lifting or bending for at least 2 weeks postoperatively. The latter measures help to inhibit graft movement and supplement the bolster’s effectiveness in minimizing shearing of the graft over its bed.
Long-term complications of FTSGs consist of cosmetic and functional problems. It is imperative to stress to the patient prior to graft placement that FTSGs usually take months to look natural. Preoperative counseling may help to alleviate fears concerning the graft’s appearance during the first weeks after bolster removal. Make-up can usually be applied 3–4 weeks after graft placement. It is important to note that FTSGs are often depressed during their first 2–4 weeks. This depression will usually correct itself within 4–6 weeks.
Although careful donor site selection will minimize the color, texture and contour deformities that can occur, patient and physician satisfaction with the cosmetic result may not be complete after healing has finished. Spot dermabrasion or laser resurfacing has traditionally been performed at 6 weeks to 6 months after grafting to correct differences in elevation between the graft and its surrounding skin, as well as to improve color and texture mismatch . While studies have focused on pulsed dye laser (PDL) treatment of postsurgical scars, not FTSGs or STSGs, a meta-analysis found an average 72% rate of improvement or no recurrence of hypertrophic scars and keloids with PDL therapy . Graft hyperpigmentation can be addressed with a brief course of topical hydroquinone and/or tretinoin.
Functional complications of FTSGs occur primarily as a result of wound contraction. Grafts contract secondary to the centripetal movement of unopposed elastic fibers. A variable amount of shrinkage can therefore be expected, depending upon donor site thickness and elasticity . In one study, it was found that the area of FTSGs contracted by a mean of 38% by 16 weeks after placement, with grafts applied to the periorbital area and nose contracting more than those on the scalp and temples . Graft contraction usually increases as graft thickness decreases, and is thought to occur in the fibrous layer under the graft, either in the bed itself or in the layer of scar tissue wedged between the graft and its bed . Complications due to graft contraction are usually minimal in FTSGs. If wound contraction does produce functional or cosmetic abnormalities, secondary revisional surgery may be needed.
Future Directions
For patients with an inadequate vascular bed, full-thickness skin grafting may not be possible, necessitating repair with a less cosmetically elegant STSG. High-density, porous, polyethylene implants have therefore been designed which permit ingrowth of fibroneovascular tissue without changing the size or shape of the implant . When these prefabricated implants were placed in rabbits, it was found that they developed sufficient vascularity to sustain FTSGs. This technology holds promise for patients with deep nasal and ear defects, in whom an anatomically correct structure could be implanted, after which, time could be allowed for fibrovascular tissue ingrowth, with full-thickness skin grafting performed later for a superior cosmetic result. Progress is also being made on incorporating complex blood vessels into bioengineered skin equivalents, and 3D printing techniques have been investigated as a possible means of generating skin equivalents. In the future, it may be possible to generate complex tissue-like constructs in a 3D pattern to use as skin grafts in facial reconstruction .
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


