Abstract
The rashes discussed in this chapter are composed of erythematous macules and papules that are widespread and sometimes confluent. Various terms have been used to describe this type of eruption, including maculopapular, exanthematous, and morbilliform (measles-like). In order to correctly diagnose generalized erythema, one must focus primarily on a complete history and physical examination, with special attention to sites of skin involvement. Skin biopsies tend to show nonspecific findings and fail to distinguish the causes of generalized erythema, except in the cases of systemic lupus erythematosus and Sézary syndrome. The majority of causes of generalized erythematous eruptions are listed in Table 14.1 in the order of relative frequency.
- 1.
Drug reactions and viral exanthems are the most common causes of a generalized erythema
- 2.
Rule out infection first in a patient with generalized erythema
- 3.
Correct diagnosis requires complete history, physical examination with attention to sites of skin involvement, skin biopsy consideration, and appropriate laboratory work-up
Drug Eruptions
- 1.
Appear suddenly and with symmetry
- 2.
Antibiotics, especially penicillins and sulfonamides, are common culprits
- 3.
Discontinuation of offending drugs leads to quick resolution
Definition
The expression: “For any rash, think drug!” reflects the finding that drug eruptions can appear similar to many inflammatory skin diseases. Think drug reaction for any symmetric rash of sudden onset. The two most common eruptions for drug reactions are hives (discussed in Chapter 16 ) and morbilliform rashes. Of these two, morbilliform rashes are more common. A morbilliform drug rash appears as a generalized eruption of erythematous macules and papules, often confluent in large areas ( Fig. 14.1 ).

Incidence
Only 0.6% of the authors’ new outpatients are seen for a drug eruption. The frequency, however, is much higher among hospitalized patients, most of whom are elderly and who receive an average of nine drugs. Drug rashes head the list for our hospital consultations and account for 7% of all dermatology consultations. It is estimated that 7% of inpatients experience an adverse drug reaction and that 2.3% of inpatients have skin reactions related to medications. Common offenders are:
- ●
Antibiotics:
- ●
β-Lactam antibiotics-penicillins, cephalosporins
- ●
Sulfonamides-trimethoprim-sulfamethoxazole (be aware of cross-reactivity with sulfonamide derivatives, especially in the following drug classes: diuretics, hypoglycemic, and antiinflammatories)
- ●
- ●
Diuretics:
- ●
Furosemide (contains a sulfonamide)
- ●
Hydrochlorothiazide (contains a sulfonamide)
- ●
- ●
Nonsteroidal antiinflammatory drugs (NSAIDs)
Approximately 2% of all medical inpatients experience drug-induced skin reactions.
History
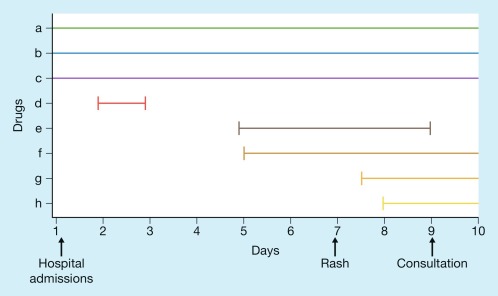
The onset of a drug-induced morbilliform eruption is usually not immediate but rather begins within several days of the initiation of the drug. Onset is sometimes delayed for as long as 1 week, but seldom longer. Because no laboratory tests are available by which to identify the responsible drug, reliance is placed on the history. For patients receiving multiple drugs, this presents a problem. In selecting a single drug from a list of many, the two variables to be considered are (1) the temporal relationship between the initiation of the drug and the onset of the rash; and (2) the likelihood that a given drug is likely to cause a drug eruption. In selecting a putative drug, it is helpful to construct a graph that depicts the patienťs drug history ( Fig. 14.2 ). In the example in Fig. 14.2 , drugs “a,” “b,” and “c” are unlikely to be implicated because the patient had been receiving these agents for months. Drug “d” was stopped 4 days before the rash began, thus making it a less likely cause. Drug “g” was started 6 hours after the rash appeared, and drug “h” was started the following day. Drugs “e” and “f” were started 2 days before the rash and therefore have the best temporal relationship. Drug “e” is a cephalosporin, a well-known cause of rash, and drug “f” is codeine, a rare cause of morbilliform eruptions. Therefore, drug “e” is the probable cause and is the first to be discontinued. Remember to include over-the-counter medications such as vitamins in your exposure list as well as PRN medications for inpatients, such as furosemide, which contains a sulfonamide, a common cause of inpatient drug reactions.
Suspect drugs that are:
- 1.
New (started within 1 week of the rash)
- 2.
Frequent offenders
| Frequency a | Etiology | History | Physical Examination | Differential Diagnosis | Laboratory Test | |
|---|---|---|---|---|---|---|
| Drug eruption | 0.6 b | Drug | Recent new drug Pruritus Usually no fever | Rash bright red and confluent | Exfoliative erythroderma (chronic) | – |
| Viral exanthem | 0.2 | Rubeola Rubella Enteroviruses, etc. | Associated “viral” symptoms | Erythema mild to moderate Mucous membranes occasionally involved | Drug reaction | Acute and convalescent viral titers |
| “Toxic” erythema | < 0.1 | Group A streptococci S. aureus Unknown | Patient feels extremely ill (“toxic”) No pruritus | Rash accentuated in flexural folds and often feels like sandpaper Mucous membranes often involved | Drug reaction | Bacterial cultures |
| Systemic lupus erythematosus (SLE) | < 0.1 | Autoimmune | Other symptoms of SLE | “Butterfly” distribution on face Sun-exposed areas favored Rarely total body | Drug reaction | Antinuclear antibody Anti-DNA antibodies Complete blood count Urinalysis |
a Percentage of new dermatology patients with this diagnosis seen in the Hershey Medical Center Dermatology Clinic, Hershey, PA.
b Frequency in outpatients. For an inpatient, a drug eruption is the most common dermatologic problem acquired in the hospital.
In patients with drug rashes, itching is usually present but is not helpful as a diagnostic marker. Fever is rarely found.
Physical Examination
The eruption is generalized and composed of brightly erythematous macules and papules that tend to be confluent in large areas. Characteristically, the erythema is intense or “drug red.” Drug rashes usually start proximally and proceed distally, with the legs being the last to be involved as well as the last to clear. See Table 14.2 for typical medications associated with other drug reaction patterns that are important to recognize clinically ( Fig. 14.3 ). It is important for the physician to recognize two, life-threatening drug reactions: (1) toxic epidermal necrolysis and (2) Stevens-Johnson syndrome. Toxic epidermal necrolysis is characterized by widespread erythema (> 30% body surface area) and full, epidermal thickness skin separation; transfer to a burn unit is critical ( Fig. 14.4 ). The erythema of Stevens-Johnson syndrome typically involves more than 10% body surface area and involves two mucosal surfaces (e.g., conjunctiva and oral mucosa); hemorrhagic crusting of the lips is pathognomonic ( Fig. 14.5 ). There is often overlap of the features with these two conditions and the authors tend be “lumpers,” not “splitters.” For practical purposes, it is important to diagnose a “life threatening drug reaction.” Both potentially fatal, drug reactions require prompt evaluation, recognition, discontinuation of offending medication, and intensive supportive care.
Drug rashes are usually:
- 1.
Bright red
- 2.
Confluent in large areas
| Type of Reaction | Drugs |
|---|---|
| Acneiform | Lithium |
| Pustules | β-Lactam antibiotics |
| Erythroderma | Allopurinol |
| Erythema multiforme, Stevens–Johnson syndrome, toxic epidermal necrolysis | Anticonvulsants, allopurinol, nonsteroidal antiinflammatory drugs (NSAIDs), sulfonamides |
| Vasculitis | NSAIDs |
| Psoriasiform dermatitis | Interferon and granulocyte colony-stimulating factor (G-CSF), tumor necrosis factor inhibitors |
| Angioedema | angiotensin-converting enzyme (ACE) inhibitors |



Differential Diagnosis
The differential diagnosis includes viral exanthem, toxic erythema, and chronic exfoliative erythroderma.
Differential diagnosis for acute morbilliform eruptions:
- 1.
Drug
- 2.
Viral
- 3.
“Toxic”
A viral exanthem and a drug eruption can be indistinguishable clinically. Often, a drug eruption is much more erythematous, more confluent, and more pruritic . The presence of viral signs and symptoms favors a diagnosis of a viral exanthem.
Toxic erythemas include scarlet fever, staphylococcal scalded skin syndrome eruptions, and Kawasaki syndrome (mucocutaneous lymph node syndrome). Features that help to distinguish these rashes from drug eruptions include a sandpaper-like texture of the “toxic” rash, mucous membrane involvement (scarlet fever and Kawasaki syndrome), the presence of fever, and a focus of infection or the presence of lymphadenopathy ( Fig. 14.6 ).

When a generalized erythema becomes chronic, it is called an exfoliative erythroderma – exfoliative because of the prominent desquamation ( Fig. 14.7 ). Long-term administration of an offending drug is one cause. The other three causes are generalization of a benign dermatosis (most often, psoriasis or atopic dermatitis), malignancy (most often, the Sézary variant of cutaneous T-cell lymphoma; see Chapter 9 ), and an idiopathic disorder.
- ●
Viral exanthema – identify cause
- ●
Toxic erythemas – identify cause
- ●
Exfoliative erythroderma

Laboratory and Biopsy
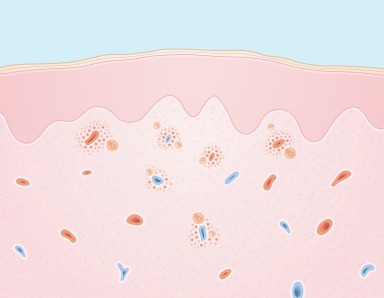
No laboratory tests can determine the diagnosis of a drug eruption or the incrimination of a specific drug. Peripheral blood eosinophilia is sometimes present and may heighten the suspicion of a drug reaction. Skin biopsy is most often performed in patients with chronic exfoliative erythrodermas. A drug eruption shows a superficial and deep perivascular inflammatory cell infiltrate ( Fig. 14.8 ). The presence of eosinophils in the infiltrate is an important clue suggesting a drug-related cause. Skin tests for penicillin may be useful for the diagnosis of immediate hypersensitivity reactions (hives and anaphylaxis) but not for morbilliform eruptions. Skin biopsies can also help distinguish the level of epidermal separation for toxic epidermal necrolysis (full thickness) versus staphylococcal scalded skin syndrome (granular layer).
Therapy
When the offending drug is identified, it should be discontinued. If the patient is taking multiple drugs and it is not possible to be certain of the offending drug, the number of administered drugs should be reduced to an absolute minimum, and any remaining possible offenders should be changed to alternative agents when possible.
Therapy otherwise is symptomatic, with antihistamines (e.g., hydroxyzine 10–25 mg four times daily) most often used for the pruritus. Moisturizing lotions are helpful during the late desquamative phase of the reaction. Topical steroids are of little value. Systemic steroids are rarely required but are helpful for the patient experiencing intense pruritus. Intensive care therapy is necessary for life-threatening drug reactions.
Initial
- ●
Discontinuance of the offending drug
- ●
Antihistamines:
- ●
Hydroxyzine (Atarax) 10–25 mg q.i.d.
- ●
Diphenhydramine (Benadryl) 25–50 mg q.i.d.
- ●
- ●
Moisturizers:
- ●
Eucerin cream b.i.d.
- ●
Alternative
- ●
Systemic steroids: Prednisone 1 mg/kg then taper dose over 7–10 days
- ●
Intensive care therapy for life-threatening reactions
Course and Complications
Drug eruptions clear slowly with time after discontinuation of the responsible agent. The time required for total clearing is usually 1 to 2 weeks. For several days after the offending drug has been stopped, the eruption may actually worsen.
Drug eruptions take 1–2 weeks to clear.
Complications are uncommon and primarily cutaneous. When large areas of skin are inflamed, increased body heat and water loss occur. In a patient already seriously ill, this could be a problem, but for most patients it is not.
One main risk of continuing an offending agent in the presence of a drug eruption involves progressive worsening of the rash, possibly eventuating in toxic epidermal necrolysis, which is characterized by the loss of large sheets of epidermis. Fortunately, this complication rarely occurs; the mortality rate for Stevens-Johnson syndrome approaches 5% and for toxic epidermal necrolysis 35%. Sometimes a drug eruption clears despite continued treatment with the offending agent, although this approach is not desirable if an alternative drug is available. If the responsible drug has been identified, the patient should be advised to avoid the drug in the future, and the medical record should be clearly labeled.
Potential consequences of continuing the offending drug – worsening rash.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


