Abstract
Cutaneous fungal infections are classified by the depth and extent of involvement: superficial, subcutaneous, and systemic. Dermatophytoses, tinea versicolor, and cutaneous candidiasis are common superficial mycoses, which are characterized by invasion of only the stratum corneum, hair, and nails. Subcutaneous mycoses such as chromoblastomycosis, mycetoma, and sporotrichosis typically result from implantation of the organism into the dermis or subcutis. Systemic mycoses may be caused by “true” or opportunistic pathogens. The former are generally dimorphic and produce infections such as histoplasmosis, blastomycosis, and coccidioidomycosis in hosts with normal immune status. In immunocompromised individuals, opportunistic pathogens can lead to primary cutaneous infections as well as systemic infections with secondary skin involvement. Worldwide, disseminated candidiasis and aspergillosis are the two most common systemic mycoses in neutropenic patients.
Keywords
fungus, tinea, dermatophyte, candidiasis, aspergillosis, Malassezia , superficial mycosis, subcutaneous mycosis, systemic mycosis, dimorphic fungi, azole antifungals, terbinafine, opportunistic fungi, tinea versicolor, pityriasis versicolor, tinea nigra, black piedra, white piedra, chromoblastomycosis, chromomycosis, mycetoma, eumycotic mycetoma, actinomycotic mycetoma, sporotrichosis, histoplasmosis, blastomycosis, coccidioidomycosis, paracoccidioidomycosis, lobomycosis, phaeohyphomycosis, hyalohyphomycosis
- ▪
Cutaneous fungal infections are broadly divided into two groups: (1) those that are limited to the stratum corneum, hair, and nails; and (2) those that involve the dermis and subcutaneous tissues
- ▪
Superficial fungal infections of the skin are most often due to dermatophytes and Candida spp.
- ▪
“Subcutaneous” mycoses are often the result of implantation, while systemic or “deep” mycoses of the skin usually represent hematogenous spread or extension from underlying structures
- ▪
In the immunocompromised host, opportunistic fungi, e.g. Aspergillus and Mucor spp., can lead to both cutaneous and systemic infections
This chapter reviews common cutaneous fungal infections, and they are subdivided into three major groups: (1) “superficial”; (2) “subcutaneous”; and (3) “deep” or systemic ( Table 77.1 ).
| ORGANIZATION OF CUTANEOUS MYCOSES | |
|---|---|
| Superficial | Involve stratum corneum, hair, or nails |
| Subcutaneous | Involve dermis or subcutaneous tissue Often due to implantation |
| Systemic (“deep”) | Involve dermis or subcutaneous tissue |
| “True” pathogens | Skin involvement usually reflects hematogenous spread or extension from underlying structures |
| Opportunistic | Primary or secondary skin lesions in immunocompromised hosts |
Superficial Mycoses
Introduction
Superficial mycoses are due to fungi that only invade fully keratinized tissues, i.e. stratum corneum, hair, and nails. They can be further subdivided into those that induce minimal, if any, inflammatory response, e.g. tinea (pityriasis) versicolor, and those that lead to more substantial cutaneous inflammation, e.g. dermatophytoses ( Table 77.2 ).
| SUPERFICIAL MYCOSES OF THE SKIN | ||
|---|---|---|
| Cutaneous disorder | Pathogen(s) | |
| Minimal, if any, inflammation | Tinea (pityriasis) versicolor Tinea nigra Black piedra White piedra | Malassezia furfur , M. globosa Hortaea werneckii Piedraia hortae Trichosporon spp. * , e.g. T. ovoides (especially of scalp hair) , T. inkin (especially of pubic hair) , T. cutaneum, T. loubieri |
| Inflammatory response common | Tinea capitis, barbae, faciei, corporis, cruris, manuum, pedis | Trichophyton , Microsporum , Epidermophyton spp. |
| Cutaneous candidiasis | Candida albicans , other Candida spp. | |
* Formerly known as Trichosporon beigelii , which has been reclassified into ~50 species, at least 16 of which have clinical relevance. Invasive or disseminated trichosporonosis typically occurs in immunocompromised patients (e.g. individuals with hematologic malignancies, organ transplant recipients) and is most often caused by T. asahii , followed by T. mucoides and T. asteroides ; in some patients, the same species is isolated from the groin. Trichosporon spp. may also occasionally cause onychomycosis and hypersensitivity pneumonitis.
Non-inflammatory superficial mycoses
▪ Tinea nigra: tinea nigra palmaris et plantaris, superficial phaeohyphomycosis ▪ Piedra: molestia de Beigel, trichomycosis nodularis ▪ Tinea versicolor: pityriasis versicolor, dermatomycosis furfuracea, tinea flava
History
In 1846, Eichstedt first noted the disease known today as tinea (pityriasis) versicolor. Over the ensuing 150 years, Malassezia furfur (previously known as Pityrosporum ovale and P. orbiculare ) came to be recognized as the causative microbe. More recently, however, studies have pointed to M. globosa as a major causative organism . In 1865, Beigel first described piedra after isolating a fungus, which was likely actually a contaminant, from a wig. Tinea nigra was first described in the 1890s by Cerqueira, who named it “keratomycosis nigricans palmaris” .
Epidemiology
Tinea nigra and piedra most often occur in tropical climates of Central and South America, Africa and Asia, but also occasionally develop in the southeastern US. While any age, ethnicity, or gender may be affected, the typical patient is a young adult. Trichosporon spp., which were previously collectively known as T. beigelii , cause white piedra and can also lead to disseminated trichosporonosis in immunocompromised individuals (see Table 77.2 ) .
Malassezia spp. are found worldwide ( Table 77.3 ). In fact, they are part of the normal flora (microbiota) of human skin (predominantly M. sympodialis, M. globosa , and M. restricta ). Although tinea versicolor occurs most frequently in tropical climates with high ambient temperatures and high humidity, it is also common in temperate climates. No racial or gender differences have been observed. Tinea versicolor favors adolescents and young adults but can occur at any age. Malassezia requires oil to grow, accounting for its predilection for sebum-rich areas of the skin. Malassezia has been implicated in several other skin diseases, including seborrheic dermatitis and atopic dermatitis, but the latter one remains controversial. Neonatal cephalic pustulosis (neonatal acne) may also be associated with Malassezia spp., particularly M. sympodialis (see Ch. 34 ).
| DIFFERENT SPECIES OF Malassezia AND COMMON CLINICAL PRESENTATIONS | |
|---|---|
| Species of Malassezia | Common clinical presentations |
| M. furfur | Tinea (pityriasis) versicolor, seborrheic dermatitis, folliculitis, neonatal cephalic pustulosis, blepharitis, and systemic infections in neonates receiving intravenous fat emulsions |
| M. globosa | Seborrheic dermatitis, tinea versicolor, folliculitis, neonatal cephalic pustulosis |
| M. sympodialis | Tinea versicolor, neonatal cephalic pustulosis * |
| M. pachydermatitis | Often isolated from domestic and wild animals; has occasionally been implicated in cases of systemic infection in humans; may play a role in chronic dermatitis and otitis externa |
| M. restricta | Seborrheic dermatitis, tinea versicolor |
| M. sloofiae | Uncommon isolate |
| M. obtusa | Uncommon isolate |
Pathogenesis
Hortaea werneckii (formerly Exophiala werneckii ) and Piedraia hortae are both environmental pathogens. H. werneckii (tinea nigra) can be found in soil, sewage, and even shower stalls under humid conditions. The source of exposure to P. hortae (black piedra) is thought to be the soil. There is no known transmission of these organisms from human to human. Trichosporon spp. (white piedra) are also acquired from the environment; in addition, they are occasionally part of the normal flora of the mucous membranes and skin, particularly inguinal and axillary areas .
Malassezia spp. normally live on human skin in amounts too minute to be detectable on potassium hydroxide (KOH) examination of stratum corneum . Tinea versicolor occurs when the round yeast form transforms to the mycelial form. Factors that can promote this conversion include high ambient temperatures and humidity, oily skin, excessive sweating, immunodeficiency, poor nutrition, pregnancy, and corticosteroid use. Because this yeast is lipophilic, use of bath oils and skin lubricants may also encourage its growth. Risk factors for Malassezia (Pityrosporum) folliculitis include chronic antibiotic use, immunosuppression, and local occlusion.
Clinical features
Piedra
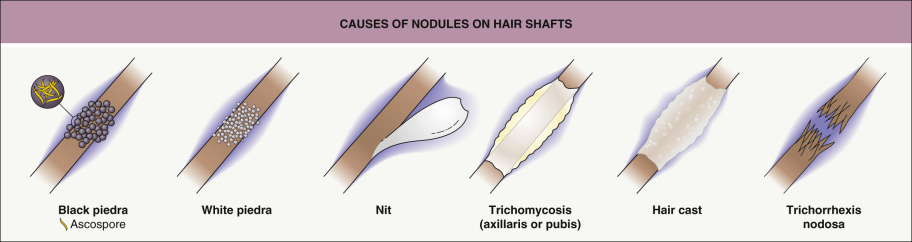
“Piedra” means “stone”, reflecting the fungal elements’ adherence to one another to form nodules along the hair shaft. Piedra is a superficial infection that begins under the cuticle of the hair and extends outward, which can lead to weakening and breakage of the hair. As the nodules enlarge, they can even envelope the hair shaft ( Fig. 77.1 ). The two major forms – black piedra and white piedra – are distinguished by their clinical appearance and findings on microscopic examination ( Table 77.4 ).
| COMPARISON OF BLACK AND WHITE PIEDRA | ||
|---|---|---|
| White piedra | Black piedra | |
| Nodule color | White (occasionally red, green, or light brown) | Brown to black |
| Nodule firmness | Soft | Hard |
| Nodule adherence to the hair shaft | Loose | Firm |
| Typical anatomic location | Face, axillae, and pubic region (occasionally scalp) | Scalp and face (occasionally pubic region) |
| Favored climate | Tropical | Tropical |
| Causative organism | Trichosporon spp. * , e.g. T. ovoides, T. inkin | Piedraia hortae |
| KOH examination of “crush prep” of cut hair shafts | Non-dematiaceous hyphae with blastoconidia and arthroconidia | Dematiaceous hyphae with asci and ascospores † |
| Culture on Sabouraud’s agar | Moist, cream-colored, yeast-like colonies ‡ | Slow-growing, dark green to dark brown–black colonies |
| Treatment | Clip affected hairs, wash with antifungal shampoo | Clip affected hairs, wash with antifungal shampoo |
* See Table 77.2 for the revised subdivision of the Trichosporon genus.
Patients with black piedra develop asymptomatic brown to black nodules along the hair shaft. White piedra manifests with soft, less adherent nodules that are typically white but may also be red, green, or light brown in color. In addition to white piedra, Trichosporon spp., especially T. asahii , can cause trichosporonosis in immunocompromised patients. This serious systemic infection presents with fungemia, fever, pulmonary infiltrates, and skin lesions. The latter are typically papulovesicular and purpuric, often with central necrosis; another potential finding is creamy white plaques resembling the in vitro fungal colonies. Trichosporon endocarditis, usually involving prosthetic valves, can also occur.
Tinea nigra
After a 10- to 15-day incubation period, tinea nigra most commonly presents as a single, sharply marginated, brown to gray–green macule or patch that can be velvety or have mild scale ( Fig. 77.2 ). There are usually no associated symptoms (i.e. pruritus), and no predisposing factors have been identified. Although most frequently seen on the palms, tinea nigra can also appear on the soles, neck, and trunk. Palmoplantar lesions are said to resemble acquired acral melanocytic nevi, but the former are usually larger, lighter in color, and lack the linear striations of acral nevi . The advancing border of a tinea nigra lesion may also be more darkly pigmented than its center. While the disease tends to be chronic, recurrence after effective treatment is infrequent except in the case of re-exposure.

Tinea (pityriasis) versicolor
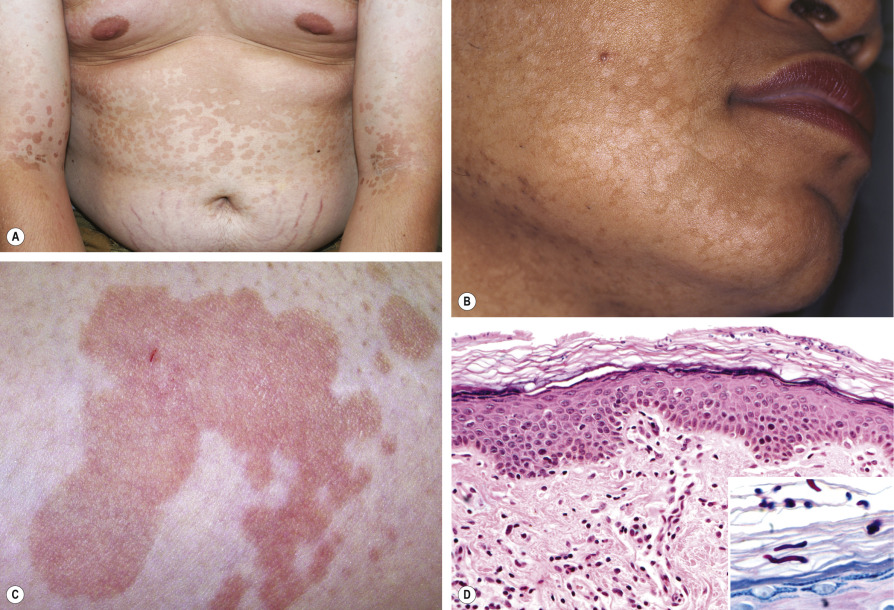
Patients usually present with multiple oval-to-round macules, patches or thin plaques with mild, fine scale. Demonstration of this associated scale may require scratching or stretching the skin surface. The lesions are often confluent centrally within areas of involvement, which may be extensive. Seborrheic regions, in particular the upper trunk and shoulders, are the favored sites. Less frequently, lesions are seen on the face (especially in children), scalp, antecubital fossae, submammary region, and groin. Involvement of flexural areas is sometimes referred to as “inverse” tinea versicolor.
The most common colors are brown (hyperpigmented; Fig. 77.3A ) and whitish-tan (hypopigmented; Fig. 77.3B ); occasionally there is mild inflammation leading to a pink color ( Fig. 77.3C ). Hypopigmentation may be secondary to either reduced tanning or inhibition of melanin production by dicarboxylic acids that result from metabolism of skin surface lipids by the yeast. In general, tinea versicolor is asymptomatic and the major concern is its appearance.
Malassezia ( Pityrosporum ) folliculitis
This condition is most commonly seen in young women and is characterized by pruritic, monomorphic follicular papules and pustules on the upper trunk, arms, neck and, occasionally, the face. It is due to excessive growth of M. furfur and M. globosa within the hair follicle, with resulting inflammation due to yeast products as well as free fatty acids generated by fungal lipases. Only yeast forms are observed, i.e. no hyphal forms as in tinea versicolor.
Pathology and fungal culture
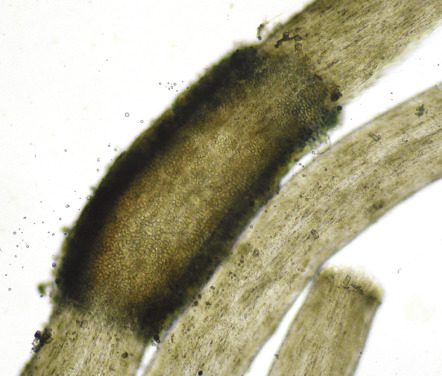
For black and white piedra, cut hair shafts are placed in KOH and a “crush preparation” is examined microscopically. In a black piedra nodule, dematiaceous hyphae are seen around an organized cluster of asci, each of which contains eight ascospores. The ascospores represent the sexual phase of P. hortae . P. hortae grows very slowly when cultured and yields a green to black colony with a velvety texture (asexual phase) .
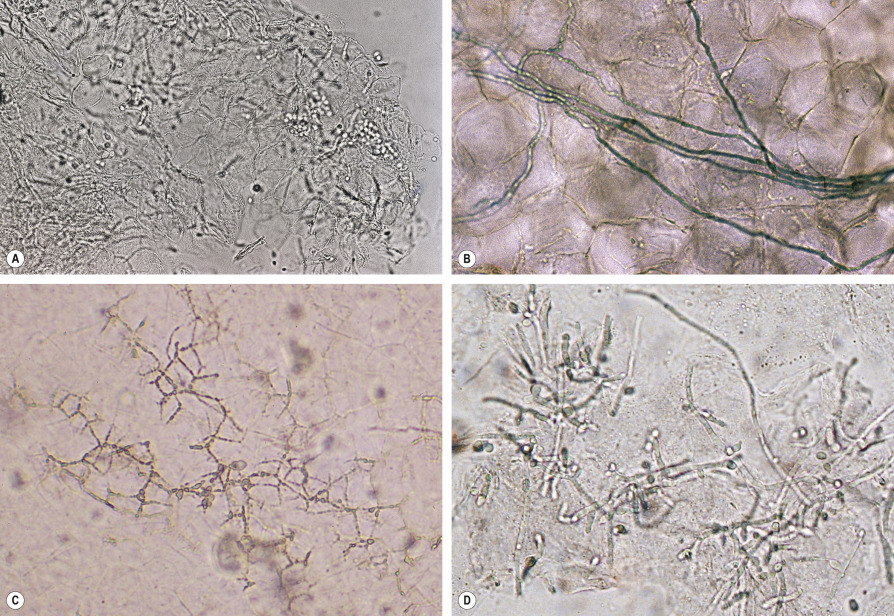
KOH preparation of a crushed white piedra nodule reveals non-dematiaceous hyphae, blastoconidia and arthroconidia, representing the asexual state ( Fig. 77.4 ). When cultured, Trichosporon spp. grow rapidly, forming moist, cream-colored, yeast-like colonies that resemble “butter cream frosting”. On Mycosel ® agar, these organisms are inhibited by the presence of cycloheximide. When Trichosporon spp. are isolated from skin and nail specimens, correlation with clinical findings is necessary to determine the medical significance.
Biopsies of tinea versicolor and tinea nigra are usually not performed, as KOH examination of associated scale is typically diagnostic. In tinea versicolor, both hyphal and yeast forms are seen; although likened to “spaghetti and meatballs”, the findings more closely resemble “ziti and meatballs” ( Fig. 77.5A ). In tinea nigra, KOH examination reveals septate pigmented hyphae. When biopsy specimens are obtained, similar findings are observed within the stratum corneum ( Fig. 77.3D ). In KOH examination of expressed follicular contents or biopsy specimens of Malassezia (Pityrosporum) folliculitis, only yeast forms are seen. Cultures of H. werneckii first appear as pasty, green–black colonies with a yeast-like appearance, and after approximately 2 weeks become a fuzzy, dematiaceous (dark in color) mold. Culture of Malassezia is generally not required; if necessary, the plate must be overlaid with sterile oil because of the organism’s lipophilic nature.
Differential diagnosis
Piedra is generally diagnosed by clinical and microscopic inspection of a hair shaft and must be distinguished from pediculosis (nits), hair casts, trichorrhexis nodosa, trichomycosis axillaris (see Fig. 77.1 ), and the scales of psoriasis and eczema. Unlike eczema and psoriasis, the scalp typically appears normal in piedra.
In most patients, the diagnosis of tinea nigra is made clinically and confirmed via KOH examination and/or fungal culture. Occasionally, tinea nigra could be confused with melanocytic nevi (see above), a fixed drug eruption, postinflammatory hyperpigmentation, or staining from chemicals, pigments, and dyes. Cutaneous melanoma has even been clinically misdiagnosed as tinea nigra.
Clinical examination is often sufficient to recognize tinea versicolor. However, pityriasis alba or other forms of postinflammatory hypopigmentation, vitiligo, seborrheic dermatitis, pityriasis rosea, tinea corporis, and secondary syphilis may be diagnostic considerations. Progressive macular hypomelanosis, which presents as non-scaly hypopigmented macules on the trunk of young adults and may be caused by Propionibacterium acnes, is often misdiagnosed as residual hypopigmentation related to tinea versicolor. Wood’s light examination revealing bright yellow fluorescence and then direct microscopy of scales can confirm the diagnosis of tinea versicolor. Malassezia (Pityrosporum) folliculitis must be differentiated from other causes of folliculitis (see Table 38.1 ), in particular itching folliculitis, as well as acne vulgaris.
Treatment
Clipping hairs with adherent nodules as well as shampooing the affected hairs with 2% ketoconazole shampoo is usually an effective treatment for piedra (see Table 77.4 ). Oral terbinafine may also be of therapeutic benefit. For treatment of tinea nigra, topical keratolytic agents such as Whitfield’s ointment (typically 6% benzoic acid plus 3% salicylic acid) are effective, as are topical azole or allylamine antifungal medications. Several weeks of therapy may be required to prevent recurrence. Systemic therapy is generally not indicated, and griseofulvin is not effective.
Tinea versicolor usually responds to topical antifungal therapy, but oral treatment with fluconazole or itraconazole can be considered when there is more extensive involvement ( Table 77.5 ; see Ch. 127 ). Residual pigmentary changes often require weeks to months to resolve. The rate of recurrence of tinea versicolor is very high, especially in hot humid climates, and maintenance therapy may be helpful (see Table 77.5 ). The treatment of Malassezia (Pityrosporum) folliculitis is reviewed in Chapter 38 .
| TREATMENT OF TINEA (PITYRIASIS) VERSICOLOR | |
|---|---|
| Initial therapy (often combination) | Topical *
Oral **
|
| Maintenance therapy to prevent recurrence |
|
* Treatment of all the skin from the neck down to the knees may lead to higher success rates.
** Although there are few comparative studies of oral antifungal medications, cure rates of 98–100% have been reported in several randomized controlled trials of itraconazole 200 mg daily × 5 days and an open-label study of fluconazole 300 mg weekly × 2 weeks.
Dermatophytoses
▪ Tinea corporis: ringworm, tinea circinata, tinea glabrosa ▪ Tinea cruris: ringworm of the groin, eczema marginatum, jock itch, gym itch ▪ Tinea barbae: tinea sycosis, barber’s itch, ringworm of the beard ▪ Tinea capitis: ringworm of the scalp/hair, tinea tonsurans, herpes tonsurans ▪ Tinea pedis: ringworm of the foot, athlete’s foot ▪ Tinea unguium: ringworm of the nail, dermatophytic onychomycosis
Introduction
Dermatophytoses are fungal infections caused by three genera of fungi that have the unique ability to invade and multiply within keratinized tissue (hair, skin, and nails). These fungi, collectively called “dermatophytes”, are alike in their physiology, morphology, and pathogenicity. The three genera are Microsporum , Trichophyton , and Epidermophyton ; species within these genera that do not invade keratinized tissue in animals or humans are not considered as dermatophytes. In naming clinical infections due to dermatophytes, “tinea” precedes the Latin name for the involved body site, e.g. “tinea pedis” refers to a dermatophyte infection of the foot. Overall, ten species of dermatophytes are commonly isolated and an additional 20 are occasionally cultured ( Table 77.6 ) .
| DERMATOPHYTES ISOLATED WORLDWIDE | ||
|---|---|---|
| Thallus (macroscopic) appearance * and/or microscopic findings | ||
| Most common | ||
| Trichophyton | mentagrophytes (previously mentagrophytes var. mentagrophytes ) | Granular front, buff reverse; pencil-shaped macroconidia, clusters of round microconidia, spiral hyphae |
| interdigitale (previously mentagrophytes var. interdigitale ) | Downy front, buff reverse; see above | |
| rubrum | White wooly front, venous blood reverse; pencil-shaped macroconidia, teardrop-shaped microconidia | |
| tonsurans | Granular front, mahogany reverse; pencil-shaped macroconidia, microconidia of varying sizes | |
| verrucosum | Convoluted, cream to gray, compact; chains of chlamydospores at 37°C | |
| violaceum | Creamy, waxy, becomes violet | |
| Microsporum | canis | White wooly front, orange reverse; multi-celled, spindle-shaped macroconidia with thick walls and rough surface |
| ferrugineum | Folded red–orange (rust-colored) front | |
| gypseum | Cinnamon–tan granular front; multi-celled, cucumber-shaped macroconidia with thin walls | |
| Epidermophyton | floccosum | Khaki green, suede to granular; beaver tail-shaped macroconidia; no microconidia |
| Less common | ||
| Trichophyton | ajelloi | Powdery surface, resembles Microsporum spp. |
| concentricum | Glabrous colonies; antler-like hyphae | |
| equinum | Club-shaped macroconidia | |
| gourvilii | Waxy, pink to red front | |
| megninii | Pink, felt-like front with red reverse | |
| schoenleinii | Glabrous; antler- and nailhead-like hyphae; rat-tail-like macroconidia (media often fissured) | |
| simii | Club-shaped macroconidia in clusters | |
| soudanense | Yellow to apricot front with fringed border | |
| terrestre | Cream to yellow granular surface | |
| yaoundei | Glabrous, chocolate-brown front | |
| Microsporum | amazonicum | Multi-celled, spindle-shaped, macroconidia with large inclusions |
| audouinii | Flat, tan front with salmon reverse; pectinate (comb-like) hyphae | |
| cookei | Oval, thick-walled macroconidia | |
| equinum | One- to four-celled macroconidia resembling M. canis | |
| fulvum | Bullet-shaped macroconidia with spiral hyphae | |
| gallinae | Diffusable pink–red pigment | |
| nanum | Two-celled macroconidia | |
| persicolor | Pink to red front and reverse, resembles T. mentagrophytes | |
| praecox | Powdery front with yellow–orange reverse | |
| racemosum | Cream-colored powdery front | |
| vanbreuseghemii | Largest macroconidia | |
History
Dermatophyte infections have been described since ancient times. In 1910, Sabouraud published a categorization scheme that is currently employed in which dermatophytes are classified by genera. However, at the time of writing, a revised and simplified nomenclature system is under review.
Epidemiology
Some dermatophytes are restricted geographically, while others are found worldwide. Trichophyton rubrum , for example, is the most common dermatophyte and has a global distribution, while T. concentricum is endemic to certain parts of the South Pacific and South America. Human travel and migration, coupled with advances in antifungal therapy, have brought about significant changes in the geographic distribution of dermatophytes. Although dermatophyte infections do occur worldwide, they are more common in tropical environments. Other important epidemiologic factors include socioeconomic status, occupation, air conditioning, and the use of footwear.
In general, dermatophytoses occur most frequently in postpubertal hosts. One major exception is tinea capitis (dermatophytosis of the scalp), which occurs primarily in children. Risk factors for the development of a dermatophyte infection during childhood include household exposure to tinea capitis or tinea pedis; environmental factors such as contaminated hats, brushes, and barber instruments; and (especially for tinea unguium) Down syndrome. Individuals with chronic mucocutaneous candidiasis, common variable immunodeficiency, or HIV infection have a propensity to develop severe, chronic, or recurrent dermatophytoses (see Ch. 60 ). Men more frequently have tinea pedis, tinea cruris, and tinea unguium than women.
Pathogenesis
Transmission of dermatophytes to humans occurs via three major sources, each resulting in infections with characteristic features ( Table 77.7 ). While dermatophytes are not especially virulent and typically invade only the outer, cornified layers of the skin, they can be responsible for considerable morbidity. The first stage of infection involves contact with and adherence of the infectious elements of the fungus (arthroconidia) to the skin. The ability of certain fungi to adhere to a particular host arises from a variety of microbial mechanisms and host factors .
| TYPES OF DERMATOPHYTES BASED ON MODE OF TRANSMISSION | ||
|---|---|---|
| Category | Mode of transmission | Typical clinical features |
| Anthropophilic | Human to human | Mild to non-inflammatory, chronic |
| Zoophilic | Animal to human | Intense inflammation (pustules and vesicles possible), acute |
| Geophilic | Soil to human or animal | Moderate inflammation |
Dermatophytes, unlike most other fungi, produce keratinases (enzymes that break down keratin), which allow invasion of the fungi into the stratum corneum. Mannans in the cell walls of dermatophytes have immuno-inhibitory effects. In T. rubrum , the mannans may also decrease epidermal proliferation, thereby reducing the likelihood of the fungus being sloughed off prior to invasion. This mechanism is thought to contribute to the chronicity of infections caused by T. rubrum . However, host factors such as protease inhibitors may limit the extent of invasion. If invasion is successful, disease occurs.
The severity of clinical disease is also affected by several host factors. Sebum has an inhibitory effect on dermatophytes, and the degree of disease activity may be related to the number and activity of sebaceous glands in a particular body region. Breaks in the skin barrier or macerated skin encourage dermatophyte invasion, and increased susceptibility related to immunologic factors may be inherited. Once dermatophytes have invaded and begun to proliferate in the skin, several mechanisms aid in limiting the infection to keratinized tissue. These include the preference of dermatophytes for the cooler temperature at the skin’s surface, serum factors that inhibit dermatophyte growth (e.g. β-globulins, ferritin, other metal chelators), and the host immune response . Further invasion or dissemination is extremely unusual (see below). Other conditions influencing dermatophyte infections include skin disorders that affect cutaneous barrier function, such as ichthyoses.
Clinical features
Tinea corporis
Tinea corporis is a dermatophyte infection of the skin of the trunk and extremities, excluding the hair, nails, palms, soles, and groin. The infection is generally restricted to the stratum corneum and most commonly affects exposed skin. Any dermatophyte can potentially cause tinea corporis, but T. rubrum is the most common pathogen worldwide, followed by T. mentagrophytes ( Table 77.8 ).
| COMMON DERMATOPHYTES THAT CAUSE TINEA CORPORIS | |
|---|---|
| Dermatophyte | Clinical features |
| Anthropophilic | |
| Trichophyton rubrum | Commonly harbored by hair follicles; may produce concentric rings; can recur; causative organism in nodular perifolliculitis (Majocchi granuloma) and most common cause of tinea corporis |
| T. tonsurans | Commonly seen in adults who care for children with tinea capitis caused by this organism |
| Epidermophyton floccosum | Generally restricted to groin, feet; responsible for eczema marginatum |
| T. concentricum | Responsible for tinea imbricata; infections typically chronic |
| T. interdigitale (previously T. mentagrophytes var. interdigitale ) | Causes interdigital tinea pedis, tinea cruris, and onychomycosis |
| Zoophilic | |
| T. mentagrophytes (previously T. mentagrophytes var. mentagrophytes ) | May be associated with dermatophytid reaction; causes inflammatory tinea pedis and tinea barbae; associated with exposure to small mammals |
| Microsporum canis | Associated with pet exposure (cat or dog) |
| T. verrucosum | May mimic bacterial furunculosis; associated with exposure to cattle |
| Geophilic | |
| M. gypseum | Frequently associated with outdoor/occupational exposure; lesions may be inflammatory or bullous |
Tinea corporis can result from human-to-human (including autoinoculation, e.g. from tinea capitis or pedis), animal-to-human (often transmitted by domestic animals), or soil-to-human spread (see Table 77.7 ). Sources include occupational or recreational exposure (e.g. military housing, gymnasiums, locker rooms, outdoor activities, wrestling) and contact with contaminated clothing or furniture .
There are multiple clinical presentations of tinea corporis, and they can mimic other dermatologic conditions ( Table 77.9 ). As with most dermatophyte infections, the extent of inflammation depends on the causative pathogen and the immune response of the host. Because hair follicles serve as reservoirs for infection, hairier areas of the body may be more resistant to treatment.
| DIFFERENTIAL DIAGNOSES OF DERMATOPHYTE INFECTIONS | ||||
|---|---|---|---|---|
| Tinea corporis | Tinea cruris | Tinea faciei | Tinea capitis | Tinea pedis |
|
|
|
|
|
The typical incubation period is 1 to 3 weeks. Infection spreads centrifugally from the point of skin invasion with central clearing of the fungus, typically resulting in annular lesions of varying sizes ( Fig. 77.6A–D ). Arcuate, circinate, concentric, and oval lesions can also develop ( Fig. 77.6D–F ). Although scale is usually present, it may be lessened or absent if topical corticosteroids have been used (tinea “incognito”). Pustules within the active border are suggestive of tinea (see Fig. 77.6E ). Lesions are occasionally vesicular, granulomatous, or verrucous ( Fig. 77.6G ). Associated symptoms may include pruritus and burning.
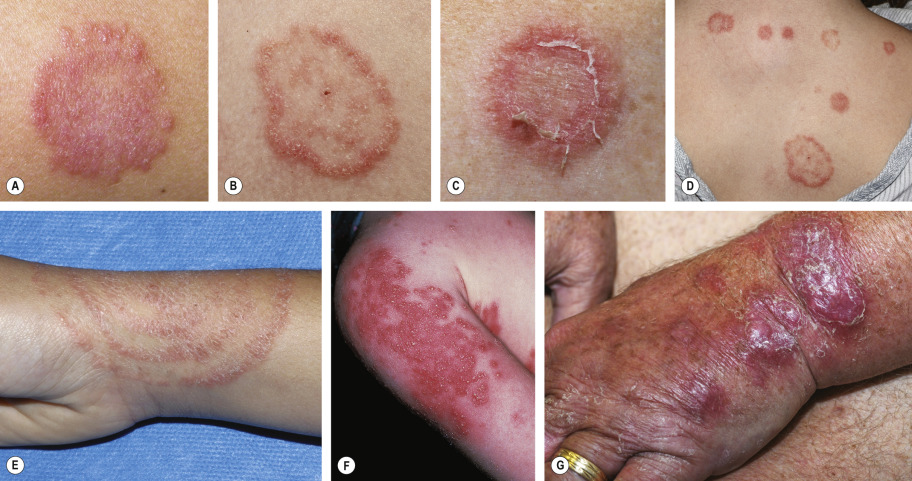
Tinea profunda, nodular perifolliculitis (including Majocchi granuloma), and tinea imbricata represent clinical variants of tinea corporis . Tinea profunda results from an excessive inflammatory response to a dermatophyte, analogous to a kerion on the scalp. It may have a granulomatous or verrucous appearance and be mistaken for cutaneous tuberculosis or a dimorphic fungal infection. Nodular perifolliculitis , usually caused by T. rubrum , is characterized by follicular papulopustules or granulomatous nodules that result from a deep dermatophyte folliculitis with disruption of the follicular wall ( Fig. 77.7 ). This variant is most commonly seen in women who have tinea pedis or onychomycosis and shave their legs, and it can also occur in the setting of immunosuppression. The lesions may be extensive or even vegetating, and a prolonged granulomatous reaction (as described by Majocchi) can develop.

Tinea imbricata is a dermatophytosis caused by the anthropophilic dermatophyte T. concentricum . It causes chronic infections in an equatorial band encompassing the South Pacific, Asia, and Central and South America. The clinical presentation consists of concentric annular rings resembling erythema gyratum repens.
Tinea cruris
Tinea cruris is a dermatophyte infection of the inguinal region, in particular the inner aspects of the upper thighs ( Fig. 77.8 ) and crural folds, with occasional extension onto the abdomen and buttocks. The three most common causative agents are Epidermophyton floccosum , T. rubrum , and T. mentagrophytes ( Table 77.10 ).

| TINEA CRURIS: COMMON CAUSATIVE PATHOGENS | |
|---|---|
| Dermatophyte | Clinical features |
| Trichophyton rubrum |
|
| Epidermophyton floccosum |
|
| T. mentagrophytes (previously T. mentagrophytes var. mentagrophytes ) |
|
This condition is more often seen in men than in women, since the scrotum provides a warm and moist environment that encourages fungal growth and men are more likely to have tinea pedis and onychomycosis as a source of dermatophytes. Other predisposing factors include obesity and excessive perspiration. Tinea cruris is frequently associated with tinea pedis because clothing that is brought over the feet is contaminated and then comes in contact with skin in the groin region.
The initial sign of infection is usually an area of erythema and pruritus in the fold between the scrotum and the inner thigh. Characteristic lesions are sharply demarcated with a raised, erythematous, scaly advancing border that may contain pustules or even vesicles. Lesions can initially be circinate and then become serpiginous. The disease may remain unilateral or become bilateral.
The duration of infection depends on the causative pathogen. Infections with T. rubrum and many other anthropophilic species tend to be chronic, sometimes with leathery and lichenified lesions. In contrast, the zoophilic form of T. mentagrophytes (previously T. mentagrophytes var. mentagrophytes ) and other animal-acquired strains often cause acute infections with a prominent inflammatory component that may include pustules and vesicles (see Table 77.10 ). The scrotum itself is generally spared in tinea cruris. If the scrotum is involved or there are erosions or satellite pustules, cutaneous candidiasis should be considered. Measures to prevent recurrences of tinea cruris include wearing loose clothing, drying thoroughly after bathing, using topical powders, weight reduction (if obese), laundering contaminated clothing and linens, and treating concomitant tinea pedis.
Tinea manuum
Dermatophyte infections on the dorsal aspect of the hand have a clinical presentation similar to tinea corporis. However, dermatophyte infection of the palm and interdigital spaces has distinct characteristics and is referred to as tinea manuum. The reason for the two different clinical pictures is thought to be related to the lack of sebaceous glands on the palms. The typical causative organisms are the same as those for tinea pedis and tinea cruris: T. rubrum , T. mentagrophytes , and E. floccosum . Infections with Neoscytalidium dimidiatum and N. hyalinum , two non-dermatophyte fungi, can have a tinea manuum-like appearance.
Moccasin-type tinea pedis is often present in patients with tinea manuum, and the two share clinical features such as chronicity and hyperkeratosis. Tinea manuum is usually non-inflammatory and often unilateral (“two feet and one hand syndrome”) ( Fig. 77.9 ; see Fig. 77.15A ); there is hyperkeratosis of the palms and digits, including within creases, that fails to respond to emollients . Tinea unguium of the involved hand can serve as a clue to the diagnosis, but infection of all the fingernails is uncommon. Other presentations include exfoliative, vesicular, and papular variants. The differential diagnosis may include psoriasis, irritant or allergic contact dermatitis, dyshidrosis, and a “dermatophytid” reaction.

Tinea barbae
Tinea barbae is a dermatophytosis that involves the bearded areas of the face and neck in men. Because the disease is often acquired from animals, the causative organisms are typically zoophilic dermatophytes, namely T. mentagrophytes and T. verrucosum . Infection with Microsporum canis or T. rubrum is uncommon. In some geographic regions, other anthropophilic dermatophytes ( T. schoenleinii, T. violaceum , and T. megninii ) are endemic and cause tinea barbae. With the increased use of disposable razors and disinfectants, the incidence of tinea due to contaminated razors in barbershops has been dramatically reduced.
Since zoophilic organisms are the most common culprit and affected areas often have a large number of terminal hair follicles, the clinical presentation tends to be severe, with intense inflammation and multiple follicular pustules. Abscesses, sinus tracts, bacterial superinfection, and kerion-like boggy plaques can develop. Patients may have constitutional symptoms such as malaise as well as lymphadenopathy and even scarring alopecia. A second type of tinea barbae is superficial, less inflammatory, and similar to tinea corporis; T. rubrum is usually the causative agent in this variant ( Fig. 77.10 ). Alopecia may be present in the center of the lesion, but it is reversible. Other conditions that can mimic tinea barbae include bacterial folliculitis, viral infections (herpes simplex or zoster), acne vulgaris, cervicofacial actinomycosis, and a dental sinus tract. Spontaneous resolution may occur if all of the infected hairs fall out.

Tinea faciei
While some dermatophyte infections of the face have classic features, e.g. scale, annular configuration, pustules in the border, others can be more difficult to diagnose clinically and require a high index of suspicion ( Fig. 77.11 , Table 77.9 ).

Tinea capitis
Tinea capitis is a common dermatophyte infection of the scalp in children ( Fig. 77.12 ), whereas adult infection occurs infrequently. The causative pathogens are members of only two genera: Trichophyton and Microsporum . T. tonsurans is currently the most common cause of tinea capitis in the US (accounting for >90% of cases), with a predilection for individuals of African descent , and M. canis is the second most frequent etiology. Globally, there is significant variation in the epidemiology of tinea capitis. While M. canis is a common cause in many countries, T. tonsurans has emerged as a major agent in Europe and elsewhere. The incidence of tinea capitis due to T. violaceum , which is endemic in Africa, has also recently increased in some areas of the US and Europe (especially western and Mediterranean regions), likely reflecting immigration patterns. The anthropophilic dermatophyte M. audouinii , which was once common and then subsequently diminished secondary to social and therapeutic advances, has more recently reappeared in Europe and may also potentially re-emerge in the US.
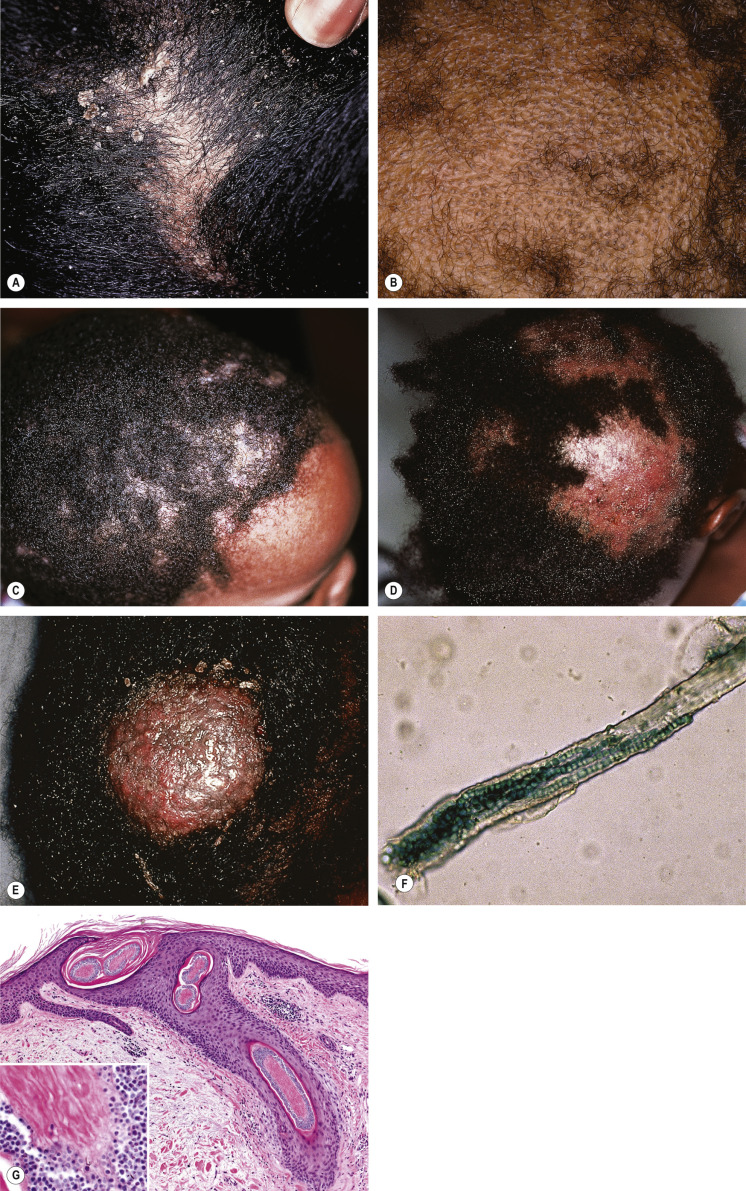
Different clinical presentations arise from the various causative organisms. For example, T. tonsurans causes an endothrix infection (see below), which classically results in “black dot” tinea capitis due to hair breakage near the scalp. In contrast, M. audouinii is an ectothrix form of tinea capitis that typically presents with dry, scaly patches of alopecia (“gray patch” tinea capitis). Both the pathogenicity of the culprit organism and the host immune response are factors that determine the severity of disease. Tinea capitis can range from non-inflammatory scaling that resembles seborrheic dermatitis (especially with T. tonsurans ; Fig. 77.12A ) to a severe pustular reaction with alopecia, known as a kerion. Alopecia with or without obvious scale is the most common presentation of tinea capitis ( Fig. 77.12B–D ). The alopecia may occur in discrete patches or involve the entire scalp. Use of dermoscopy can highlight “comma”, “corkscrew”, and dystrophic broken hairs that represent clues to the diagnosis of tinea capitis (see Ch. 69 ) . Many patients have posterior cervical and posterior auricular lymphadenopathy, which is helpful in differentiating tinea capitis from less inflammatory causes of alopecia, such as alopecia areata.
A kerion results from advanced disease coupled with an exaggerated host response that leads to boggy, purulent plaques with abscess formation and associated alopecia ( Fig. 77.12E ). Some patients may even become systemically ill with extensive lymphadenopathy. The hair in the affected area usually returns, but the longer the infection persists, the more likely the alopecia will be permanent. If a kerion is misdiagnosed as a bacterial abscess and treated with antibiotics following incision and drainage, the infection will likely worsen, thereby increasing the likelihood of scarring alopecia.
The “carrier state” of T. tonsurans refers to a clinical situation in which there are no obvious signs or symptoms of a scalp infection, yet a positive fungal culture is obtained. Although also seen in children, this typically occurs in adults who have been exposed to infected children. The carriers shed the fungus and are considered contagious . Consequently, some experts advocate treating all carriers with oral or topical antifungals.
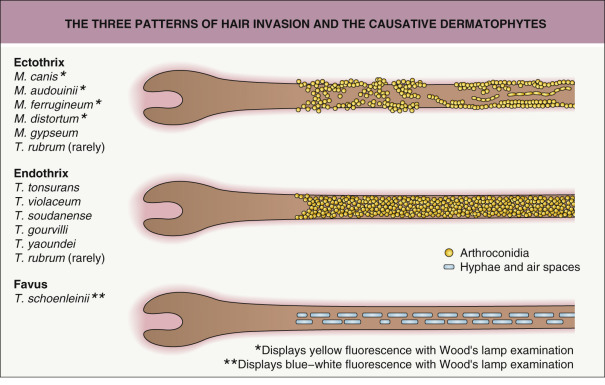
For those dermatophytes that invade hair, three patterns of invasion exist: endothrix, ectothrix, and favus ( Fig. 77.13 ):
- •
The endothrix pattern results from infection with anthropophilic fungi in the genus Trichophyton and is characterized by non-fluorescent arthroconidia within the hair shaft ( Fig. 77.12F ). The clinical presentation varies from scaling to “black dots” with patchy alopecia to kerion formation. T. tonsurans and T. violaceum are important causes of endothrix infection.
- •
The ectothrix pattern occurs when arthroconidia are formed from fragmented hyphae outside the hair shaft (see Fig. 77.13 ). Cuticle destruction ensues. Ectothrix infection can be fluorescent ( Microsporum ) or non-fluorescent ( Microsporum and Trichophyton ), as determined by Wood’s lamp examination. Clinical features vary from patchy, scaly alopecia with little inflammation that may mimic alopecia areata to kerion formation.
- •
Favus is the most severe form of dermatophyte hair infection and is most frequently caused by T. schoenleinii . Hyphae and air spaces are observed within the hair shaft, and a bluish-white fluorescence by Wood’s light examination is typically seen. Favus presents as thick, yellow crusts composed of hyphae and skin debris (“scutula”). Scarring alopecia may develop in chronic infections ( Fig. 77.14 ).

Fig. 77.14
Favus due to Trichophyton schoenleinii .
Scarring alopecia with erosions and several scutula on the occipital scalp. The latter represent masses of keratin plus fungi.
Courtesy, Israel Dvoretzky, MD.
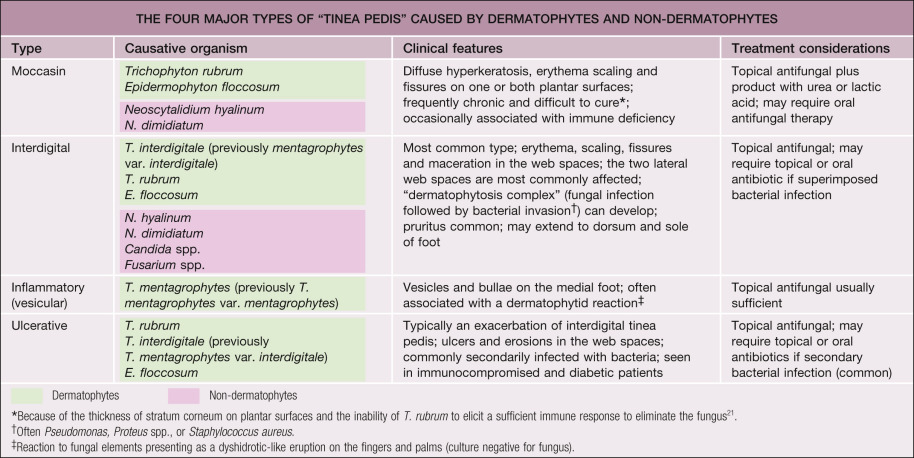
Tinea pedis
Tinea pedis is a dermatophyte infection of the soles and interdigital web spaces of the feet. Infection of the dorsal aspect of the foot is considered tinea corporis. The feet are the most common location for dermatophyte infections, and the majority of the US adult population has experienced tinea pedis. This condition is more common in adults than children and is found around the world, affecting both sexes. The lack of sebaceous glands and the moist environment created by occlusive shoes are important factors in the development of tinea pedis . In fact, tinea pedis is uncommon in populations that do not wear shoes. However, the fungus may be acquired from going barefoot (locker rooms, gyms, public facilities).
The dermatophytes that are typically responsible for tinea pedis are T. rubrum , T. interdigitale (previously T. mentagrophytes var. interdigitale), T. mentagrophytes , E. floccosum , and T. tonsurans (in children). Non-dermatophyte pathogens that produce clinical findings identical with tinea pedis include Neoscytalidium dimidiatum and N. hyalinum (moccasin and interdigital types) and, occasionally, Candida spp. (interdigital type). There are four major clinical types of tinea pedis, as outlined in Table 77.11 : moccasin ( Fig. 77.15A ), interdigital ( Fig. 77.15B ), inflammatory ( Fig. 77.15C ), and ulcerative. Each type has different associated morbidities and complications that can affect diagnostic considerations and therapeutic options. These include bacterial superinfection (the “dermatophytosis complex”), dermatophytid reactions, cellulitis (especially in patients who have venous hypertension, harvested saphenous veins, and chronic edema), and even osteomyelitis leading to amputation in diabetics. Other conditions that can mimic tinea pedis are listed in Table 77.9 . KOH examination and culture easily differentiate the moccasin and inflammatory forms of tinea pedis from these entities . Erythrasma can be diagnosed with Wood’s light examination because of its “coral red” fluorescence. Oral antifungal therapy should be considered in diabetics, immunocompromised patients, and those with moccasin-type tinea pedis. Finally, other dermatophyte infections often occur together with tinea pedis – in particular, tinea cruris, onychomycosis, and tinea manuum – and these sites should be examined ( Fig. 77.16 ).