Introduction
Reconstruction after partial mastectomy is an evolving aspect of plastic surgery. Different modalities are continually being developed to maximize patient survival while minimizing the treatment’s morbidity. Currently, the two main options for the management of primary breast cancer are total mastectomy and lumpectomy with radiation. Due to advances in imaging and treatment algorithms, complex partial breast deformities are more and more common.
Breast conservation therapy (BCT) may be considered a mainstay therapy for early stage breast cancer and an oncologic equivalent to mastectomy. The most important difference that was identified between BCT and mastectomy was a significantly higher rate of local recurrence after BCT. This was, however, only found in a minority of the randomized controlled trials, , , and the differences are of questionable relevance to current practice given the lack of microscopic margin control in those trials. In recent literature, although confounding by severity and residual confounding cannot be excluded, better long-term breast cancer specific survival is showed for BCT than mastectomy. With more contemporary diagnostics and therapies, several subgroups may benefit from BCT.
Even in patients with locally advanced breast cancer (LABC) first treated with neoadjuvant chemotherapy (NCT), the prevalence of local recurrence after breast conserving surgery (BCS) was 9.2% versus 8.3% in the mastectomy group, without significant difference. The 5-year local recurrence-free survival (LRFS) rate was lower in the mastectomy group than in the BCS group, but no significant difference was found between the two groups. So we can conclude BCS after NCT to be safe in terms of local recurrence and LRFS even in LABC. Shrinking tumors with NCT provides the opportunity to apply BCS with no detriment to outcome. BCT might be preferred in most breast cancer patients when both BCT and mastectomy are suitable. BCT comprises partial breast resection, lymph node dissection, and whole breast irradiation. No breast cancer subgroup can be spared postoperative radiation after BCT.
Although the oncologic outcome is well defined, the ultimate aesthetic outcome after BCT remains highly variable. Conventional reports in the radiation oncology literature indicate unsatisfactory appearance in more than a third of patients following BCT at late reporting by patients or radiation oncologists. In fact, 50% of post-BCT aesthetic results were only considered to be fair or poor when assessed by a plastic surgeon. In relative terms, the size of the tumor excision must be compared with the size of the affected breast to estimate the final aesthetic impact. The larger the breast, the more easily it accommodates larger resections up to a certain size. Small to medium breasts are far less tolerant of increasing resection sizes than large breasts. Cosmetic outcome after BCT is influenced by breast and tumor size and axillary lymph node dissection (ALND). Although several reconstructive options are available, the optimal method for revision surgery has not yet been determined. Future studies are necessary to obtain evidence-based guidelines for reconstructive surgery after BCT.
Oncoplastic surgery is a combination of breast conservative surgery and partial breast reconstruction. There is an unmet demand for partial breast reconstruction both immediate and delayed, with an opportunity to advocate and increase awareness on behalf of patients undergoing BCT. The number of patients requiring partial breast reconstruction can be comparable to the number of patients looking for reconstruction after skin-sparing mastectomy.
Timing of Partial Breast Reconstruction
Despite the established role of free flaps in breast reconstruction after mastectomy, their role in partial breast reconstruction is not well defined. This chapter reviews the use of free flap techniques for immediate, delayed-immediate, and delayed partial breast reconstruction. Most reconstructive surgeons believe that immediate reconstruction provides superior aesthetic outcomes with fewer complications; however, it is important to be aware of the rate of re-excisions for positive margins by the surgeons performing the tumor resections. If this rate is unacceptably high, then reconstruction should be delayed. Our preference is to perform immediate reconstruction with either breast remodeling (displacement techniques) or pedicled flaps (replacement techniques). Clinical outcomes and expert opinions support this approach. These sources suggest that post-BCT breast contour deformities are primarily due to a surgical defect that is inappropriately corrected and secondarily from the injury induced by radiotherapy. Radiotherapy tends to exacerbate the surgically created deformity. Utilizing the principles of oncoplastic surgery, the aesthetic impact of BCT can be minimized by filling the unfavorable resection cavity with local or distant tissues before administering radiation. Immediate reconstruction has definite advantages over delayed reconstruction, as lower complication rates and substantially more straightforward corrections can be expected because the surgical field has not received prior irradiation with its widespread implications for tissue injury and scarring. The possibility of including free flaps in the armamentarium of the plastic surgeon performing partial breast reconstruction allows the oncologic surgeon to do wider excisions and avoid reinterventions for positive margins or local recurrence. In addition, it provides the freedom to offer BCT to patients in situations where the defect is expected to be significant.
An alternative to immediate oncoplastic surgery is “delayed-immediate” reconstruction, where the reconstruction is performed after final pathology clearance but before radiation. This approach may be more suitable when volume replacement techniques are required using pedicled flaps; However, it must be the standard approach when free flaps are used. The use of a free flap for immediate partial breast reconstruction has been scarcely described in literature. Many plastic surgeons feel that sacrificing the best available tissue for total breast reconstruction such as the abdominal free flaps is not ideal for immediate or delayed-immediate partial breast reconstruction for a variety of reasons. Free flaps are a more demanding procedure and are often difficult to be combined with lumpectomy because of logistic and organizational issues. Moreover, it is more beneficial for the patient to keep this option available when required for salvation in case of recurrence and subsequent need for mastectomy or failure of BCT. Therefore, the focus of this chapter describing the use of free flap options will only be in situations of delayed reconstruction.
Indications of Delayed Partial Breast Reconstruction
If immediate reconstruction is not performed in cases with unfavorable resection defects, significant breast deformities will likely manifest following completion of the BCT regimen. These deformities, volume loss, distortion and fibrosis, have been stratified by two major classifications. Berrino et al were the first to classify post-BCT deformities by identifying the morphology of the deformity and then referencing this to select a technique for correction. They described the following deformity types: (I) displacement of the nipple–areolar complex (NAC), (II) localized deficiency of parenchyma and/or skin, (III) generalized breast contracture with no localized defects, and (IV) severe damage with heavily scarred parenchyma and skin. Clough et al have altered this classification by reordering and combining groups, emphasizing reconstructive choices and including comparison with the opposite breast. They classified BCT deformity into three types that include: (I) deformity of the affected breast with no contour defects and leading to asymmetry with the contralateral breast, (II) deformity requiring delayed partial reconstruction, and (III) severe deformity requiring mastectomy and whole breast reconstruction. In clinical applications, these classifications help to clarify the deformities that typically result when BCT is performed under suboptimal conditions. The classification schema also guides us in reconstruction with emphasis on identifying what is missing or disordered, and on seeking a reasonable match between the two breasts.
When these post-BCT deformities occur, delayed partial breast reconstruction must be considered. We consider these cases to be difficult and fraught with potential problems on three separate fronts. First, these patients often present to us with ongoing disappointment about their breast appearance and with higher cosmetic expectations than when they were in the primary cancer treatment phase. Second, breasts previously treated with BCT present limited options for reconstruction due to reduced breast volume, scarring, distorted anatomy, and disturbed vascularity. Third, post-radiation changes must be approached with caution, as correction is technically difficult and results in complications that are highly unpredictable. Studies have estimated the complication rate to be as high as 50% and the final aesthetic result to be poor when extensive tissue rearrangement is performed in the previously irradiated breast. Due to these serious concerns, we limit post-BCT reconstruction to contralateral symmetrisation procedures, ipsilateral local flaps, or scar revisions requiring minimal dissection of the affected breast. Specific ipsilateral options include importing of distant tissues using pedicled or free flaps, as well as lipofilling to correct the skin and/or parenchymal deficiencies. Before performing delayed partial breast reconstruction, an oncologic update consisting of physical examination and breast imaging is required to confirm the absence of recurrence.
Patient Selection
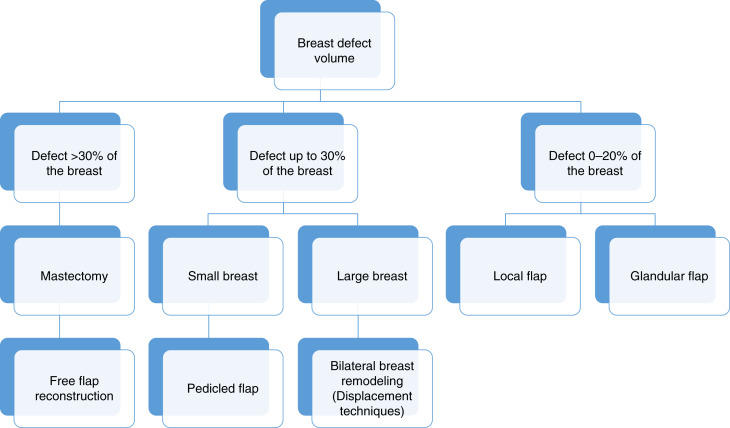
The success of the oncoplastic procedure depends on the size of the cancer, the anatomical position, and the volume of resection needed to achieve clear margins in relation to the volume of the breast. The choice of the technique used depends on many factors, including the extent of resection, the time of surgery, the breast size and tumor location, and patient preferences ( Fig. 11.1 ).
With BCT, the NAC is usually preserved, but a significant number of patients have resulting deformity and asymmetry. There are two fundamental surgical techniques for partial breast reconstruction: volume displacement and volume replacement. In contrast to volume displacement techniques, volume replacement techniques are technically more difficult and are typically used in patients with a low body mass index (BMI) with small- to moderate-sized breasts or when the tumor-to-breast ratio is large and the remaining breast tissue is insufficient for adequate tissue rearrangement. Volume replacement with the use of non-breast local or distant flaps provides both tissue for the filling of the glandular defect and the skin deficiency of the reconstructed breast.
Preoperative History and Considerations
Surgeons performing free flap techniques for partial breast reconstruction should consider the aesthetic subunits, anatomical landmarks, and breast proportions and shape to achieve a pleasing outcome. Preoperative evaluation of the patient and her breasts must be standard and detailed.
The examination must include:
- •
General quality of the breast: evaluation of breast skin, elasticity, thickness, scars, and any defining marks such as tattoos, stretch marks, contour irregularities, and previous breast surgery and/or radiation
- •
Palpation for masses or abnormalities in the breast parenchyma, nipple inspection, and detailed documentation of breast sensation
- •
Breast shape, volume, position, grade of ptosis
- •
The base and width of the breast, the width of the NAC, the height of the nipple, and the distance from the sternal notch, midline, and inframammary crease
- •
The NAC position or distortion
- •
Number and location of affected quadrants
- •
Status of the contralateral breast
- •
Different body types, skin laxity, and fat distribution are important factors in the decision-making process of free flap selection
Preoperatively, incision lines and preservation of the NAC should be discussed with the oncologic surgeon and patient. The estimation of the defect size after tumor resection and breast size-to-tumor ratio is a guideline to the choice of the reconstructive method. Immediate correction of asymmetry by a contralateral mastopexy or reduction should also be discussed ( Table 11.1 ).
Preoperative evaluation should include the same work-up as for any other free flap autologous breast reconstruction technique. On physical examination, the skin of the donor site region is inspected for scarring, previous incisions, and estimation of tissue bulk with a pinch test.
Indications and Contraindications
Our algorithm for recruiting distant tissues for partial breast reconstruction is to turn first to pedicled flaps and then to free flaps if pedicled flaps are insufficient or unavailable. Conventional pedicled flap options include the latissimus dorsi (LD) muscle or myocutaneous flap and the transverse rectus abdominis myocutaneous (TRAM) flap. These have been shown to be perfectly suitable for breast reconstruction following irradiation, with the accepted caveats of higher complication rates and poorer aesthetic results. The muscular component of the flaps is transferred in a denervated state, so any attempt to utilize muscle for parenchymal replacement must include substantial overcorrection to account for future denervation atrophy. Despite good results with the TRAM flap, we strongly discourage its use for partial breast reconstruction due to concern that this tissue may be needed in the future for reconstruction in the event of completion mastectomy for local breast cancer recurrence, or after primary mastectomy for cancer of the contralateral breast. With the development of pedicled perforator flaps for partial breast reconstruction, more options and lower donor site morbidity through muscle-sparing are now available when a large amount of tissue is needed.
A particular anatomical limitation to the use of pedicled flaps for partial breast reconstruction must be noted. Laterally based pedicled flaps (i.e., LD, lateral intercostal artery perforator (LICaP), thoracodorsal artery perforator (TDaP)) generally are not suitable for reconstruction of large defects of the medial breast quadrants due to insufficient reach and intervening healthy breast tissue. Although this is a recognized limitation, only a few reports acknowledge this. The TRAM reaches the medial breast quadrants easily; however, its use for partial breast reconstruction must be discouraged because this eliminates the use of the abdominal wall flap for a local recurrence or a new tumor in the contralateral breast as previously discussed. In addition, there is the risk of donor site morbidity such as a bulge or hernia. A solution for the donor site morbidity might be the use of a superior epigastric artery perforator (SEaP) flap; however, this still utilizes the abdomen that may be needed in the future.
Another option for women with smaller breasts is to use retropectoral implants in conjunction with tissue rearrangement. However the frequent use of postoperative radiation in patients undergoing BCT increases the risk of capsule contracture. For medial defects, it will also be quite difficult to position the implant correctly. Also there is no replacement of skin with this approach.
Among the limited indications for free flap reconstruction of partial breast defects we find patients who are likely to have a poor cosmetic result of BCT, due to high tumor/breast ratio or medially or inferiorly based tumors. In the senior author’s experience, indications for free flaps are genuine but limited to delayed free flap reconstruction of partial mastectomy defects that include:
- •
Severe breast deformity (Clough Grade III) when non-abdominal pedicled flaps are inadequate or unavailable (e.g., large need for skin replacement).
- •
Large breast deformity (Clough Grade II) in the medial quadrants.
- •
In conjunction with completion mastectomy for difficult tumor control or major glandular fibrosis postirradiation (Berrino Grade IV).
- •
As part of treatment consisting of contralateral mastectomy (therapeutic or prophylactic) and correction of ipsilateral post-BCT deformity.
- •
With aesthetic abdominoplasty procedure in a patient with long term follow-up and no further risk of recurrence or developing a new breast cancer.
- •
After prior mastectomy and immediate flap reconstruction with unsatisfactory results due to tumor recurrence or fat necrosis following radiotherapy
In the delayed correction of a post-BCT deformity, whenever a free flap is an option, completion mastectomy should be considered, especially in patients with a high probability of subsequent cancers (multicentric disease, BRCA mutations, strong family history, suspicious magnetic resonance imaging findings on contralateral breast, unfavorable cancer oncotype) or patients who have a history of prior radiation therapy. The goal of the reconstructive procedure is to provide breast symmetry in an oncologically safe manner. Partial breast reconstruction is sometimes required in non-oncologic cases to correct congenital or secondary breast deformities.
Operative Approach
Principles
The principles of using free tissue transfer for post-BCT deformity are summarized in Table 11.2 .
Preoperative Planning
- •
Thorough preoperative consultation is essential to explain the surgical plan, expected results, and potential high complication rate due to the post-radiotherapy status. Furthermore, every candidate for this technique should undergo a complete history and physical examination by the oncology team before considering an attempt at surgical correction. This examination must be comprehensive and should encompass the entire body including the breasts. Magnetic resonance imaging of the breast is considered when there is ambiguity in the interpretation of the preoperative mammogram or ultrasound examinations.
- •
The patient is usually marked the day before surgery. The breast size, defect size, and location are estimated.
- •
Preoperative computed tomographic angiography (CTA) images of the donor site and thoracic region are routinely obtained for perforator mapping and recipient vessel evaluation. After the flap markings and the grid localization of the perforating vessels are completed according to the anticipated defect, the location of the dominant perforator is confirmed with a unidirectional handheld Doppler.
- •
Good communication between teams, oncologic and reconstructive, is mandatory.
- •
It is important to understand the importance of blood supply to the nipple, placement of skin incisions, and to have an appreciation of breast aesthetics.
- •
It is equally important that the reconstructive surgeon appreciate the size and location of the tumor, margin status following excision, and the need to ensure locoregional control.
- •
Both surgeons should review the radiographic imaging, discuss the anticipated defect location and size, as well as whether or not the resection will include skin. This will assist with determination of the most appropriate glandular pedicle required to maintain nipple viability and reshape the mound.
- •
- •
Anticipate a back-up plan, as occasionally the defect is different from that anticipated, and an alternative approach may be required. The incisions for the tumor resection are based on optimizing oncologic excision as well as reconstructing an aesthetically pleasing breast.
- •
Immediate partial breast reconstruction should be delayed if the surgeon is uncertain about the margins or tumor extension (e.g., tumors with large in-situ component) despite the preoperative radiological assessment. A delayed immediate reconstruction can still be safely performed within a few days following determination of the definitive margin.
Free Flap Selection
- •
Flap planning should account for what is missing from the breast skin and parenchyma but also should consider the reduced elasticity in the residual breast tissue. In a free flap reconstruction, an ample and adequate skin paddle should be available with proper planning. Usage of free flaps also facilitates orientation of the skin paddle. In our flap plethora, we consider perforator flaps to be the gold standard for reconstruction because of their low donor site morbidity.
- •
Our first choice is the deep inferior epigastric artery perforator (DIEaP) flap ( ). It provides an ample amount of soft tissue with good color and consistency match. The superficial inferior epigastric artery (SIEa) flap is a good alternative to the DIEaP flap whenever the direct cutaneous SIE vessels are available and suitable in diameter to perform safe flap transfer. Therefore, the lower abdominal incision is made first to assess to availability of the SIE vessels. Because the abdominal donor site can only be used once, its use for partial breast reconstruction makes it unavailable in the future for whole breast reconstruction; therefore, its use should be evaluated very carefully. In some patients, the quantity of abdominal tissue is insufficient for total breast reconstruction; thus it may be more suitable for partial breast reconstruction. Another argument supportive of the DIEaP flap is that, in body contouring surgery, this tissue is often discarded in a population that is at higher risk for breast cancer compared with the risk of a recurrence in adequately treated breast cancer after BCT. The cosmetic result obtained by removing excess tissue from the abdominal area coupled with minimal donor site morbidity and a well-concealed scar make abdominal flaps an attractive option for partial breast reconstruction. Some patients view the opportunity to improve their overall appearance as an overwhelming benefit of free abdominal perforator flap surgery.
- •
The transverse myocutaneous gracilis (TMG) flap has become a valuable alternative in absence of availability of abdominal perforator flaps. For bilateral reconstruction cases, TMG is in particular a good option due to the easy accessibility of both donor sites without need for repositioning. Another option is the Profunda artery perforator (PaP) as well as medial circumflex femoral artery perforator (MCFaP) flaps that have also been used to reconstruct medial quadrant lumpectomy defects.
- •
Other alternative flaps include the superior gluteal artery perforator (SGaP) and inferior gluteal artery perforator (IGaP) flaps that may also be considered for post-BCT reconstruction. However, in cases of bilateral free flap breast reconstruction, simultaneous SGaP or IGaP reconstruction is time-consuming due to the multiple repositioning of the patient that is required. In our institute, bilateral gluteal flap surgery is usually performed in two stages with a 3–6-month interval between stages.
- •
A free LD myocutaneous flap has been reported as a salvage option for partial medial breast reconstruction after partial loss of a free TRAM flap. To limit donor site morbidity, we advocate the use a thoracodorsal artery perforator (TDaP) flap.
- •
Omental flaps have been used as a pedicled flap for medial quadrant defects and as a free flap for lateral defects. However, due to the difficulty of predicting the flap volume, problems in harvesting the flap in patients with previous abdominal surgery, and the lack of a skin island, in our hands the use of this flap for partial breast reconstruction is rare.
Surgical Technique
- •
During surgery, all damaged skin, scar, and fibrotic tissue is excised. Frozen section examination can be requested if recurrence is suspected within the excised tissue. A completion subcutaneous mastectomy can be performed. Thicker skin flaps are developed, with preservation of internal mammary perforators to the medial breast tissues. This maximizes vascularity and thereby minimizes ischemic slough of the previously irradiated skin. We believe that, by performing a completion subcutaneous mastectomy, a significant reduction in the cancer recurrence rate and a more complete release of the postirradiation parenchymal fibrosis can be achieved. Patients can be reluctant to sacrifice the remaining breast tissue or lack the adequate donor tissue for whole breast reconstruction. Another reason to preserve the internal mammary artery perforator (IMaP) vessels is to have the option to perform microanastomosis on these vessels that may be more adequate as recipient vessels based on size and position in certain flaps compared with the internal mammary artery and vein.
- •
The mastectomy skin should be treated with great care, especially after previous radiation. Lengthening an incision is preferable to traumatizing the skin with retractors that may result in skin flap necrosis. If there is any doubt on skin flap viability, peroperative evaluation of perfusion can be performed using indocyanine green technology.
- •
The recipient vessels should be carefully prepared if irradiation was delivered specifically to the selected region. The internal mammary vessels and their branches are preferred because these vessels usually have less damage following radiation when compared with the thoracodorsal vessels. In addition, sparing the thoracodorsal vessels allows for the future use of a pedicled TDaP or LD flap for breast salvage in the case of free flap failure or cancer recurrence. The internal mammary vessels are usually prepared without removing rib cartilage.
- •
After harvesting the free flap and performing the microanastomosis, the flap inset is completed with a larger skin paddle than the original breast skin deficiency. The flap skin paddle ideally replaces an entire breast aesthetic subunit rather than leaving a small and poorly concealed patch that is very conspicuous when viewed alongside the native breast skin. The flap inset and shaping is performed with the patient in a seated position to match the cavity. Flap inset in partial reconstructions has some particular challenges that include:
- •
Variability of the defect location, shape, and size
- •
Different positioning of pedicle and recipient vessels
- •
Limited skin incision results in a more challenging flap inset and also inhibits a clear view of the anastomoses following inset. The use of an implantable Doppler probe on the vein should be considered when visualization of the pedicle is not possible and the flap has to be inserted through a small incision. A limited incision with tight skin can result in flap compression and limit venous drainage, which may be difficult to identify when there is only a small skin island.
- •
In flaps that include a small segment of muscle, future muscle atrophy and reduction in flap volume should be anticipated; therefore, initial flap volume should be oversized. In immediate or delayed-immediate reconstruction volume loss due to radiotherapy should also be considered. Other options in achieving symmetry in the future include liposuction and/or lipofilling, excision, and/or contralateral reduction. Although irradiated flaps are less tolerant for liposuction.
- •
Donor site closure should be performed with great care. Closing the abdomen, thigh, or gluteal region should be performed with the same attention as in an aesthetic body contouring. Attention to these details will make the difference between a nicely healed and well-accepted scar or result in another stigma and reminder of cancer surgery.
Postoperative Care
- •
Patients are administered low molecular weight heparin (LMWH) during the time of relative immobilization for prophylaxis against deep venous thrombosis.
- •
Patients typically are discharged from the hospital when the drains are removed, on average about 5 days after surgery.
- •
A compression garment is applied over the donor site for approximately 6 weeks postoperatively.
- •
When immediate reconstruction is performed, adjuvant irradiation of the breast, if indicated, can be started at 6 weeks post-reconstruction. Adjuvant chemotherapy can start 3 weeks postoperatively. This type of reconstruction rarely results in a delay starting adjuvant therapy.
Related posts:
 Indications and Patient Selection for Oncoplastic Breast Surgery
Indications and Patient Selection for Oncoplastic Breast Surgery
 Reduction Mammaplasty and Oncoplastic Surgery
Reduction Mammaplasty and Oncoplastic Surgery
 Oncoplastic Breast Surgery and the Effects of Radiation Therapy
Oncoplastic Breast Surgery and the Effects of Radiation Therapy
 Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
Plastic Surgeon’s Approach to Oncoplastic Breast Surgery
 Surveillance and Imaging Following Oncoplastic Breast Surgery
Surveillance and Imaging Following Oncoplastic Breast Surgery
 Volume Displacement and Volume Replacement Techniques
Volume Displacement and Volume Replacement Techniques
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


