Key points
- •
Understand the attributes which characterize fractionation of laser delivery.
- •
Understand the immediate tissue effects of fractionated treatments.
- •
Know the differences between ablative and non-ablative fractionated laser treatments.
- •
Understand appropriate parameter selection for different indications.
- •
Learn to manage appropriate pre- and post-care.
Introduction
An understanding of the performance of current fractionated laser treatments requires a review of the antecedent treatments which led to their development. The introduction of laser resurfacing using scanned and pulsed CO 2 laser systems was initially designed to provide tissue ablation with what was thought to be minimal thermal effect, just enough to achieve hemostasis. In fact, CO 2 laser resurfacing treatments produced clinically significant residual thermal damage. This became rapidly evident for a number of reasons. Firstly, histology of affected tissue showed clear zones of thermal damage deep to the ablated tissue. Secondly, the degree of clinical improvement in wrinkles was much more pronounced several months after a resurfacing treatment compared to after initial healing, including a substantial degree of skin tightening. Thirdly ‘hotter’ carbon dioxide lasers that created more tissue desiccation provided more tightening and more thermally induced complications. Fourthly, the introduction of erbium:YAG resurfacing treatments with substantially less residual thermal damage showed less clinical improvement and much less skin tightening at initially applied parameters. Subsequent changes in laser parameters for Er:YAG resurfacing changed this but the experience showed the importance of thermally induced biological stimulation to tissue remodeling in obtaining substantial results.
Despite the success of laser resurfacing, the drawbacks of open wounds with the attendant wound care, risk of infection and patient discomfort as well as the substantial risk of pigment disturbance led to a search for alternative technologies. Simply put, the clinical improvement from laser resurfacing can be divided into two broad categories of effects. The first is tissue removal, which provides the mainstay of clinical improvement. This results from ablation of tissue with an evening of the hills and valleys of the wrinkles or acne scars. The second is due to a thermally induced inflammatory response causing the area to continue to tighten and smooth for a period of months. This results from the body’s response to tissue that is thermally altered but not removed. A progressive increase in the density and organization of collagen in the dermis is observed in the months following laser resurfacing.
This biological response to the laser resurfacing wound raise the question of whether a treatment could be devised that would stimulate the remodeling response discussed above without removing or ablating tissue or creating an open wound with all the associated risks and inconveniences. Essentially, the goal of this nonablative remodeling (also called subsurface remodeling) treatment as it came to be called was to separate the two modalities of clinical improvement and rely solely on remodeling without any tissue removal. Several strategies were devised utilizing a laser pulse of energy directed to the mid-dermis with a synchronized cooling application to protect the epidermis and upper dermis from injury.
Over a period of months after a series of these non-ablative treatments, a degree of skin smoothing would theoretically result. The difficulty that became apparent after these treatments were adopted by the clinical community related to the degree of biological response that could predictably be obtained. Tissue removal in an ablative laser process is very predictable and reproducible. There is very little variation from patient to patient. Non-ablative remodeling techniques obtained their clinical result not from the physical effect of the energy application with the laser but from the ensuing biological response. This response varies tremendously from patient to patient. By definition, patients seeking wrinkle treatments have skin in which youthful maintenance mechanisms are at least somewhat diminished. What this means in clinical practice is that some patients are non-responders deriving no readily discernible clinical benefit from non-ablative remodeling treatments even if biopsies might reveal biological changes in their skin. The remainder of responding patients will get a range of improvement from modest to more pronounced. Unfortunately, no useful criteria have been developed which predict which patients will benefit. Positive attributes of the non-ablative remodeling treatments include very low risk of pigment complications in the skin and little or no recovery associated with each treatment.
Frustrations with the unpredictable outcomes associated with non-ablative remodeling treatment and the undesirable recovery associated with ablative laser resurfacing led to the development of fractional treatments as an extension of this approach. The skin surface is exposed to a succession of thousands of microscopic beams of light each of which is separated from the neighboring beams whether applied sequentially or simultaneously. The skin underlying each small beam of light was coagulated but not ablated. By limiting the diameter of the wounds created and the total percentage of skin exposed in a single treatment, the depth of treatment could be extended safely to less than that which was associated with scarring in classical wounds. The limited nature of the tissue injury and the large reservoir of unwounded tissues surrounding each area of exposed tissue allow rapid healing with a minimum of risk compared to all preceding photothermal laser therapies. There has been considerable research performed as to how the MTZ heal. They appear to extrude the desiccated tissue from the surface leaving behind rejuvenated collagen.
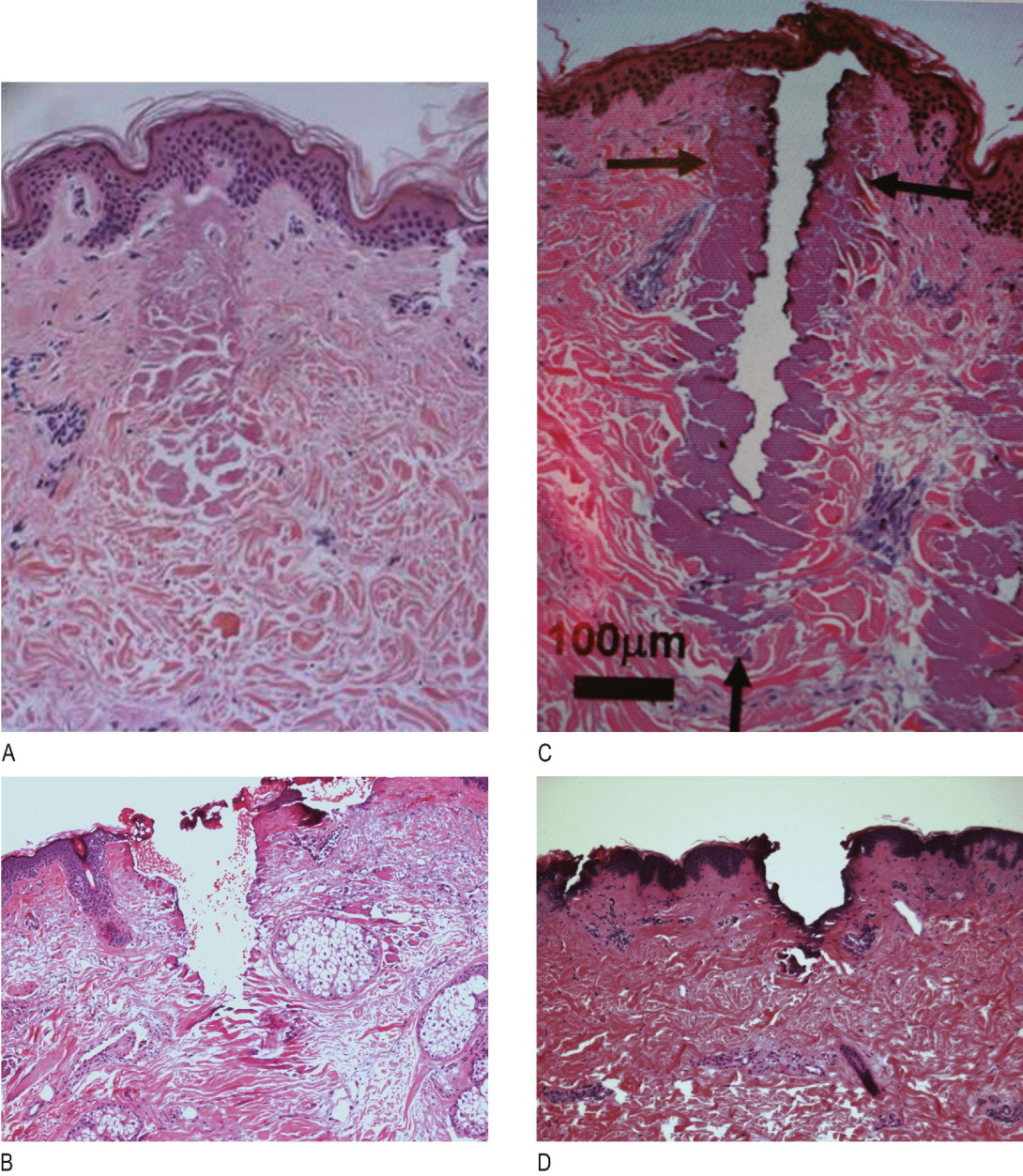
A fractionated treatment has the fundamental attribute that only a portion or fraction of the treatment zone is exposed in any single laser treatment. Small beams of light are used to expose the skin to light energy. These small beams produce a zone of exposed tissue underlying the area of skin that they impinge called microthermal zones (MTZ). These MTZs represent a column of tissue which is treated by the laser light to the target endpoint or endpoints for the light energy ( Figure 4.1A ). In between the areas of exposure are areas of unexposed tissue. By exposing only a fraction of the tissue in the target area, several advantages can be obtained. The exposed skin can heal more quickly with a large volume of unexposed tissue surrounding it to act as a reservoir or source of cells to heal the exposed tissue. Treatments can extend to depths that would heal poorly or with scar if performed as a conventional field treatment. Areas that heal more slowly than the face can be safely treated using fractionated treatments due to the faster healing and high risk cases can often also be treated safely. Despite this, the procedure still has risks and must be properly performed and managed in order to obtain reliable results.
The downside of non-ablative fractional resurfacing is that multiple treatments are needed to see good clinical results. In some cases, five to six treatments are used per patient. As treatments are performed 2–4 weeks apart and collagen may take many months to rejuvenate the final results may not be seen for several months after starting treatment. Needless to say, there are many patients who wanted quicker results but were not able to commit to the downtime of full field resurfacing.
The need for quicker results has led to a parallel development of ablative fractional resurfacing. Carbon dioxide and erbium wavelengths are available with others such as YSGG to come ( Figure 4.1B,C ). The interesting point to be made is that the discussion of efficacy between erbium and carbon dioxide is the same as that which took place in the past for full field resurfacing, namely that carbon dioxide devices create more thermal damage and have increased downtime compared to erbium devices. When fractional erbium and carbon dioxide histology is compared there are ablation channels created with both devices with the carbon dioxide devices having more adjacent thermally damaged tissue. At the time of the writing of this chapter there have been no direct comparisons of erbium to carbon dioxide fractional devices in terms of efficacy although proponents of the carbon dioxide devices claim greater tightening albeit with greater downtime. This led to the development of variable pulse width erbium fractional devices that produce more thermal damage than short-pulse width devices. ( Figure 4.1D ) The long-pulse is created with a train of pulses and histology shows increased thermal response as more trains are added. Early clinical work with this device shows more tightening than with the short pulse device with minimal changes to downtime.
A number of details of parameter selection from fractionated devices may influence results including spot size, depth, density and thermal damage. However, there is a distinct lack of clinical studies that address these. First, the sizes of the light beam must be relatively small. Typical fractionated devices have spot sizes in the range of 75–750 µm. How large the spot size can become while preserving the rapid healing of skin even with deep treatments is unclear but is likely to be 750 µm or less. Early work by the authors compared three spot sizes for fractional erbium lasers including round 250µm, round 750µm and square 430µm and failed to show a difference in healing times between these spot sizes.
Results were similar but may be slightly better with the larger spot sizes. Second, spacing between laser exposures must be preserved to some degree. Some of these fractionated treatments place multiple passes with the potential for some overlap and increased depth and a confluence of peak thermal effects which is undesirable. Clinical experience shows that depth of non-ablative fractional resurfacing needs to be deeper than with ablative devices to see clinical results. Quantification of this is not known at this time. Increased density or closeness of ablation channels appears to improve results and increase downtime. Optimal density is not known and its relationship with spot size not known. Adequate energy must be available in each exposure to obtain the desired depth of effect for the indication being treated. Preferred parameters vary depending on the indication for the treatment and the particular device selected. The role of thermal damage as discussed above needs further elucidation. Downtime is clearly related to parameter use. For ablative and non-ablative fractional devices increasing depth and density will increase recovery period.
Indications
Each available fractionated device bears its own regulatory approvals for different clinical indications. However, devices that have appropriate parameter capability could be reasonably expected to provide some efficacy for the range of indications commonly employed by fractionated lasers of that specific wavelength or absorbing chromophore. Some laser systems may not have an appropriate spot size or adequate energy to provide the necessary tissue effects despite the fact that the laser energy delivered by these devices is delivered simultaneously or sequentially as multiple small beams of light.
Common indications for fractionated lasers in the near and mid-infrared range include treatment of acne scars, hypertrophic scars, and traumatic scars. Many effects of photoaging can also be treated including particularly rhytids and solar lentigines and to a lesser extent skin laxity and vascular changes (e.g. telangiectasias). Specifically melasma but also other pigment disorders that manifest both superficial and deep placement of pigment are amenable to correction. Any other indication that would be improved by skin resurfacing could also potentially benefit from these treatments.
Nearly every type of laser or light-based treatment is being re-examined to determine if it would benefit from fractionated delivery. The indications, efficacy and advantages of this approach are unproven, though promising, for these other application areas.
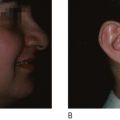
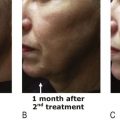
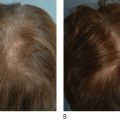
Patient selection
Any patient presenting for the indications listed above can benefit from these fractionated laser treatments. Non-ablative fractionated resurfacing produces less wrinkle correction on average than field ablative laser resurfacing, and likely produces less than ablative fractionated resurfacing which is too new as of this writing to judge long-term results. For treatment of rhytids, non-ablative fractionated treatments are appropriate for patients who are willing to undergo a larger series of treatments in order to obtain a minimum of downtime and can accept a lesser degree of response ( Figure 4.2 ). It is not clear that non-ablative fractionated resurfacing patients receive any significant degree of improvement in skin laxity although isolated individuals may receive some benefit. Other patients who would benefit from non-ablative fractionated treatments include those with melasma or other pigment disturbances or patients at high risk for post-inflammatory hyperpigmentation. Until the advent of ablative fractionated treatments, non-ablative fractionated resurfacing was the treatment of choice of one of the authors (LB) for acne scars and traumatic scars.