Chapter 15 Flexor Tendon Injuries in Children
Outline
Pediatric flexor tendon injuries remain a complicated problem for the hand surgeon. The factors that contribute to the difficulties in treating these injuries in children include difficulties in diagnosis, the technical demands of the repair, and the child’s compliance with postoperative therapy. Five decades ago, more than 90% of flexor tendon injuries in children were missed at the time of the initial injury and thus were treated late with flexor tendon grafting.1 Unfortunately, within the present day, a significant percentage of flexor tendon injuries in children still present late making primary repair more difficult. Reasons for continued delays in identification of these injuries include difficulties or inadequacy of physical examination. Many flexor tendons injuries in children are due to lacerations with broken glass, which may produce a small skin laceration or puncture but is often associated with a high rate of injury to underlying vital structure.2
Advances in flexor tendon repair techniques and the introduction of early postoperative rehabilitation protocols have improved the results of flexor tendon surgery in adults over the last two decades.3–7 Unfortunately, these advances are not always applicable to children with flexor tendon injuries due to the size of their tendons and their compliance with therapy. The size of the profundus tendon can be less than 4 mm in young children, making the placement of multiple core sutures difficult, particularly if larger suture material is used. Finally, early motion protocols can result in flexor tendon rupture if the child is noncompliant with splinting or therapy. The purpose of this chapter is to review the pertinent issues in the management of flexor tendon injuries in children, including clinical pearls for identification, repair, and rehabilitation of these injuries in an effort to improve outcomes of flexor tendon injuries in this age group.
Incidence
Finger flexor tendon injury in the pediatric population is less frequent than in adults. In a report from Helsinki, the annual incidence is 3.6 per 100,000 children (<16 years). Peak incidence is at 7 years of age. The ratio of boys to girls was 3:1.8 Broken glass is the most common mechanism of injury with some authors reporting nearly 80% of such injuries being caused by it.9–12 As in adults, zone 2 injuries are the most common injuries in children with the little finger being the most commonly injured.10,13,14 The rate of concurrent digital nerve injury range from 36% to 58%.8,11,12,14–16
Diagnosis
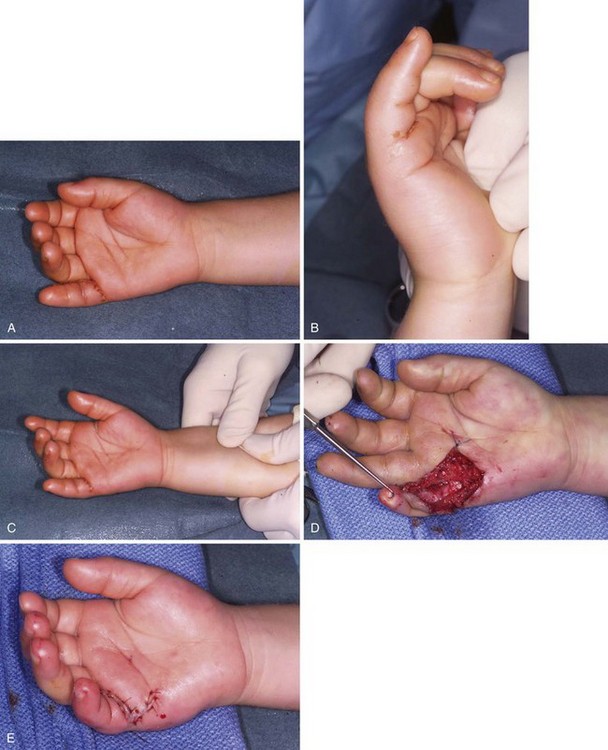
The assessment of flexor tendon injuries in the pediatric population is difficult (Figure 15-1). Young children, particularly those under 6 years of age, cannot be expected to cooperate well with the examiner during the hand exam.1 Observation and additional techniques must be used to determine the status of the flexor tendon in children. Previous reports by Bell and Mason have also noted the importance of observation of the child’s hand at rest and during play to look for signs of active flexion or a loss of the normal cascade within the hand.1,9 Children with older injuries will learn to adapt to their injury and can gasp the injured finger with a normal adjacent finger during flexion, thereby giving the impression that active motion is being performed.1 This trick maneuver, called “trapping,” may initially mislead both parents and examiners into thinking that there is no disability.13
Missed diagnosis resulting in a delayed diagnosis still accounts for 15% to 30% of pediatric patients with flexor tendon injuries.8,11,14 The risk of delayed diagnosis and treatment is particularly high in children who are less than 6 years of age8 and, paradoxically, in children who sustain injuries with small surface wounds that bleed little.1 Wounds that bleed profusely often compel parents to seek medical attention and the likelihood of a missed flexor tendon injury is thus lower. Regardless, a high index of suspicion should always be adopted when faced with a child with a hand or finger laceration.
Examination begins with simple observation of the resting posture of the hand. In the normal situation, the fingers of the hand lie in a cascade with some flexion being present in all the finger joints. A finger that is observed to be out of alignment from the normal finger cascade may have a flexor tendon injury. If the joints in that finger are carefully observed, it may be possible to even determine which flexor tendon is injured. In complete lacerations of both the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) tendons, both the proximal interphalangeal (PIP) joint and distal interphalangeal (DIP) joint will be extended. In isolated lacerations of the FDP tendon, only the DIP joint will be in extension with residual flexion present in the PIP joint. In isolated FDS injury, the finger will lie out of the normal finger cascade but there will be residual flexion present in both the PIP and DIP joints. If the child permits, the tenodesis effect can be elicited by performing passive wrist flexion and extension to check for integrity of the flexor tendons (Figure 15-2). In a normal situation, one should observe increasing flexion of all finger and thumb joints with passive wrist extension. Assuming that the child is cooperative and is able to relax, flexor tendon injury should be suspected if there is either absence of flexion or decreased amount of flexion in a finger joint. Passive flexor tendon excursion can also be performed by compression of the flexor tendons in the distal forearm. Again, if there is absent flexion or decreased amount of flexion, this would suggest a complete flexor tendon laceration (see Figure 15-1C).

Radiographs of the injured finger or hand may be useful in excluding a retained foreign body or underlying fracture. Ultrasound has limited diagnostic accuracy in an uncooperative child. Magnetic resonance imaging (MRI) is expensive and requires a general anesthetic for young children.13 Both modalities can be considered if the child is sedated.
Examining for digital nerve injury in the child can be virtually impossible if they are not able to understand or cooperate with the examination. As such, the usual methods employed in the adults such as comparative light touch and two-point discrimination tests may not work. Thus, in children, nerve injury should always be suspected based on the location of the surface wound. The loss of resistance to glide using a plastic pen can help in diagnosing the loss of sweating in a nerve injury. Alternatively, the hand may be immersed in water at room temperature until skin wrinkling occurs. As only innervated skin wrinkles, an area of unwrinkled skin indicates a likely nerve injury.13 In older injuries, dryness or trophic changes are clues to sensory nerve disturbances.1 Surgical exploration under anesthesia may be the only way to verify the condition of the nerves.9,13
Treatment
Related posts:
 Gene Therapy for Tendon Healing
Gene Therapy for Tendon Healing
 Treatment of the Flexor Tendon Sheath and Pulleys
Treatment of the Flexor Tendon Sheath and Pulleys
 Tendon Friction, Lubrication, and Biomechanics of Motion
Tendon Friction, Lubrication, and Biomechanics of Motion
 Staged Tendon Grafts and Soft Tissue Coverage
Staged Tendon Grafts and Soft Tissue Coverage
 Outcomes of Flexor Tendon Repairs and Methods of Evaluation
Outcomes of Flexor Tendon Repairs and Methods of Evaluation
 Customizing Flexor Rehabilitation Based on Zone or Type of Injury
Customizing Flexor Rehabilitation Based on Zone or Type of Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


