Chapter 22 Outcomes of Flexor Tendon Repairs and Methods of Evaluation
Outline
The well-recognized importance and challenges in flexor tendon repair in the hand are reflected in the number of the past investigations (publications) relating to this subject. The inaugural issue of the widely read Hand Clinics was devoted to flexor tendon repair. Twenty years later, in the preface of the second issue of Hand Clinics for flexor tendon repair in 2005, Daniel Mass and Craig Phillips wrote that this controversial complex topic “has produced more articles in the peer-reviewed hand literature than any other single topic.” It is true that flexor tendon repairs have been and remain one of the hottest topics in hand surgery. The reports of outcomes of primary repair of the injured flexor tendons were sporadic before the 1980s, because this practice had not become the mainstay of surgical repair of the injury in the early and middle of the last century. From the 1980s up to the recent years of this century, we have seen a great number of reports1–31 that document the outcomes of primary, or delayed primary, tendon repair, end-to-end surgical tendon repair methods and evolving postsurgical rehabilitation methods.
Outcomes Over the Past 20 Years
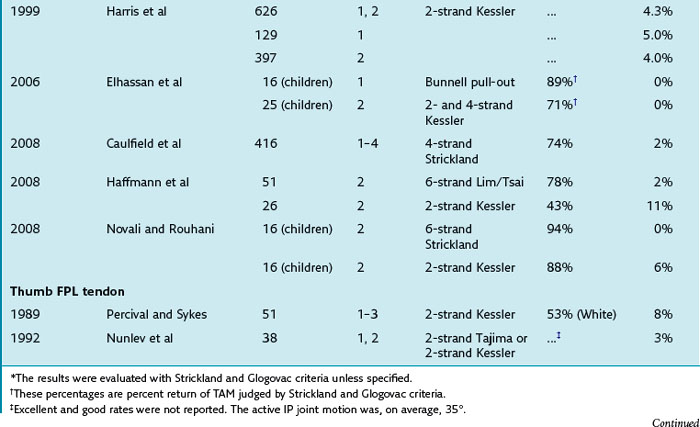
I reviewed the outcomes of primary tendon repair in a 2005 article in Hand Clinics.1 An updated review of the outcomes of flexor tendon repairs in fingers and thumb over the past 20 years (1989–2009) is provided in Table 22-1.
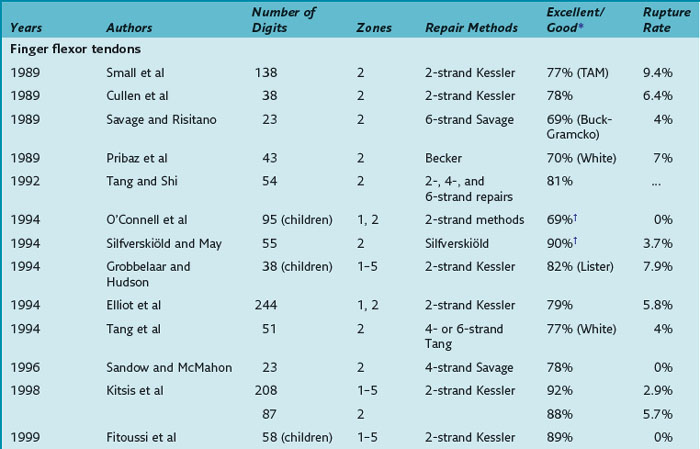
A few important observations can be summarized from an analysis of outcomes over this period (as well as the results presented in Chapter 13):
1 Good or excellent recovery of function from the centers involved (which are among the leading hand surgery units treating flexor tendon injuries) were in around three-fourths, or 75% of the cases.
2 The most common method of quantifying outcomes is the original Strickland and Glogovac method.
3 Primary or delayed primary tendon repairs were prioritized over secondary repair by all surgeons.
4 Early tendon motion, either passive or active (or combined), was advocated in all cases by surgeons and participating therapists, except for children.
5 Early active motion regimens were adopted in the late 1980s, initially producing a high rate of repair rupture (around 10%) with conventional (weaker) two-strand repairs, which has been a great concern.
6 There has been a gradual but clear shift from using two-strand core suture repairs to stronger four- or six-strand surgical repairs, or to use stronger peripheral repair since 1990s.
7 Use of stronger surgical repairs has lowered rupture rates, but in most reports, ruptures have not been eliminated, with 2% to 4% rupture rates frequently recorded.
8 Over the past decade, more surgeons have adopted (and reported) some type of early active motion regimen, together with use of stronger surgical tendon repairs.
9 New tendon repair materials (such as fiberwire) emerged, and surgeons have reported good functional outcomes and fewer repair ruptures with fiberwire repair.
10 Multiple methods are currently used to evaluate and record the outcomes of tendon repair. Some worldwide consensus on methods of recording outcomes is necessary to facilitate comparisons of results.
Major Reports and Important Information
Over the past 20 years, a number of excellent clinical reports have highlighted some important facts regarding primary flexor tendon repairs. In 1989, The Journal of Hand Surgery (British Volume) simultaneously published clinical reports of primary tendon repairs with controlled early active tendon motion by Small et al,2 Cullen et al,3 and Savage and Risitano.4 Small et al2 presented 114 patients with 138 zone 2 flexor tendon injuries treated over a 3-year period. Ninety-eight patients were followed and graded using the total active range of motion (TAM) method of the American Society for Surgery of the Hand (ASSH). The active range of motion was graded excellent or good in 77% of the digits, fair in 14%, and poor in 9%. Repair rupture occurred in 9.4% of the fingers (11 digits). The ruptured tendons were re-repaired immediately and a similar early motion program was applied. Cullen et al3 treated 34 adult patients with 70 zone 2 flexor tendon injuries in 38 fingers; 78% fingers were rated excellent or good by the original Strickland criteria after a mean follow-up of 10 months. Two tendons ruptured during active finger flexion exercise. Savage and Risitano4 used their six-strand method of repairs to treat flexor tendon lacerations in 36 fingers followed by protective active finger flexion exercise; 63% of lacerations were zone 2 and 27% were zone 1, and 69% and 100% (respectively) achieved an excellent or good result using Buck-Gramcko’s assessment method.
Silfverskiöld and May5 reported outcomes of use of an innovative strong peripheral suture (cross-stitch epitendinous suture) combined with a modified Kessler core suture in treatment of flexor tendon injuries in zone 2 in 55 digits among 46 patients. For the first 4 weeks after surgery, fingers were mobilized with a combination of active extension and passive and active flexion. Repair ruptures occurred in two tendons. Six months after surgery, the mean TAM of the distal and proximal interphalangeal (DIP and PIP, respectively) joints in the remaining fingers was 63° and 94°, respectively. Elliot et al11 reported 233 patients with complete divisions of the flexor tendons in zones 1 and 2. Their cases included 203 patients with 224 finger injuries (317 divided flexor tendons) and 20 patients with 30 complete divisions of the flexor pollicis longus (FPL) tendon. The patients were treated with a controlled active motion regimen postoperatively. Repaired tendons ruptured in 13 (5.8%) fingers and 5 (16.6%) thumbs. In follow-up of the patients treated during the last year of the study, 10 (62.5%) of 16 fingers with zone 1 repairs and 50 (79.4%) of the 63 fingers with zone 2 repairs were rated good or excellent using the original Strickland and Glogovac criteria.
Emphasis on the need and application of strong (four- or six-strand) core repairs in clinical tendon repairs appeared first in Savage and Risitano’s report4 in the late 1980s, followed by the report of Tang and Shi7 and Tang et al7,12 in 1992 and 1994 and then a series of reports in Atlas of the Hand Clinics by Taras et al,13 Sandow and McMahon,14 and Lim and Tsai15 in 1996. In 1992, Tang and Shi7 reported the results of treatment of 72 flexor tendon injuries in zone 2 in primary or delayed primary stages; 80.4% of the fingers were rated good or excellent results on assessment by the Strickland and Glogovac criteria. Among 72 tendons, 32 tendons were repaired with four- or six-strand core sutures using looped sutures, together with simple peripheral stitches. In 1994, Tang et al12 reported 51 fingers from 46 patients with zone 2 flexor tendon lacerations. Doubled threads of the looped suture were placed to repair injured flexor digitorum profundus (FDP) or superficialis (FDS) tendons, or three threads of the looped suture to repair the FDP tendons. The results were good or excellent in 76.5% using White’s criteria. They reported two repair ruptures (4%) during the postoperative motion program. Taras et al13 used double-grasping Kessler-type core and cross-stitch peripheral sutures in repairing 21 flexor tendons (three FPL, four FDP in zone 1, and 14 FDS or FDP in zone 2) of 14 digits. The patients underwent active finger flexion motion initiated on the first postoperative day, including place-and-hold exercise three times weekly under supervision. Between therapy sessions, a standard elastic-thread traction passive flexion and active extension program was maintained. Overall recovery of digital motion was graded as excellent in 12 and good in 2. The seven fingers with FDP and FDS repairs in zone 2 averaged 83% recovery of motion. Sandow and McMahon14 reported 37 FDP tendons in zones 1 to 5 using a modified single-cross six-strand repair based on the original Savage method followed by early active tendon motion. Of 23 zone 2 tendon injuries in 18 patients, 78% were rated as good or excellent using the Strickland and Glogovac criteria, with no ruptures or need of secondary surgery. Lim and Tsai15 used six-strand tendon repairs with looped suture to repair the tendon injuries in zone 2 with good functional outcomes.
Several other reports also provide interesting and important information about tendon repairs. Kitsis et al16 reported results of treatment of 339 flexor tendon repaired with two-strand modified Kessler core suture and a Halsted peripheral suture in zones 1 to 4 of 208 fingers. The important message from this large case series is that among 6 ruptures of the repaired tendons, 5 occurred in zone 2 and one in zone 5. Repair rupture was most frequent in zone 2 and the rupture rate was 5.7%. Harris et al18 reviewed the results of 728 primary zone 1 and zone 2 flexor two-strand modified Kessler core suture tendon repairs in 526 fingers of 440 patients. A total of 23 fingers (6 in zone 1 and 17 in zone 2) ruptured 28 tendon repairs. One hundred twenty-nine fingers with zone 1 injuries had a rupture rate of 5% (6 fingers) and 397 fingers with zone 2 injuries had a rupture rate of 4% (17 fingers). The ruptures occurred in 6 tendons within the first week, 5 in the second week, 6 in the third week, 5 in the fourth week, 3 in the fifth week, and 1 in the tenth week. An important message from this case series is that rupture can occur anytime from the first week to the tenth week after surgery. The “dangerous period” is postsurgical weeks 1 to 6, and postoperative week 2 is not associated with a higher incidence of repair ruptures than week 1 or weeks 3 to 6. More recently, Dowd et al19 analyzed the results of immediate re-repair of zones 1 and 2 flexor tendon repairs that rupture during postoperative early motion exercise. The outcomes of the re-repair of the ruptured tendons were generally poorer than the primary repairs, but function of re-repaired tendons were still clinically acceptable, with 9 (24%) excellent, 10 (27%) good, 5 (14%) fair, and 13 (35%) poor when assessed by the Strickland and Glogovac criteria out of a total of 37 fingers with re-repair of the tendon.
In 2008, The Journal of Hand Surgery (European Volume) published a series of reports on flexor tendon repairs using stronger core tendon sutures (multistrand core sutures) combined with early active flexion exercise.20–22 These reports indicate lower rupture rates among tendons with strong core tendon repairs but also illustrate that it is not always possible to avoid repair ruptures. Caulfield et al20 reported 416 tendon repairs in zones 1 to 4 repaired with a four-strand Strickland core suture in 272 patients. The results were 74% good or excellent graded by the Strickland criteria, with only 2% repair ruptures. They had identical outcomes using absorbable and nonabsorbable sutures. Hoffmann et al21 reported 51 fingers of 46 patients undergoing zone 2 flexor tendon repair using the Lim/Tsai repair method combined with a Kleinert and Duran early motion regimen and place-and-hold exercises. Repair rupture occurred in 1 (2%) of 51 repaired fingers. Two (4%) fingers required tenolysis. In the cases they treated with the two-strand modified Kessler repair and the Kleinert and Duran motion regimen alone, they had repair ruptures in three fingers (11%) and tendon adhesions, or dehiscence, in three fingers (11%), which required secondary surgery. The good or excellent outcome rate was 78% with the Lim/Tsai method and 43% with the two-strand Kessler method. Navali and Rouhani22 reported on 32 flexor tendon repairs in zone 2 of 29 children using either the two-strand modified Kessler method (16 tendons) or the four-strand Strickland method (16 tendons). They achieved good or excellent outcomes in all fingers, except one rupture and one fair outcome among the tendons with the two-strand repair and one fair outcome in the tendons with the four-strand repair.
In children, repairs of flexor tendons produced generally good or excellent results. Early motion exercise is not essential for a tendon to regain a good range of active motion. These observations were validated in reports by Elhassan et al23 in 2006 and by Navali and Rouhani22 in 2008.
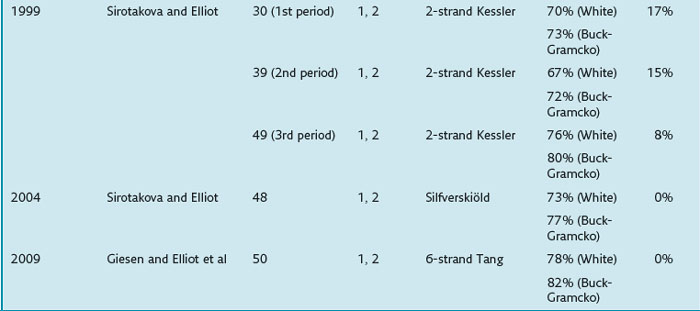
Repair of the FPL tendons is usually discussed separately from flexor tendon repair in the fingers.24–31 Sirotakova and Elliot27,30 analyzed the results of primary repairs of the FPL tendon followed by early active motion with only the thumb splinted. The first 30 patients were repaired with a Kessler suture and simple epitendinous suture. The later 49 patients underwent repair with a Kessler suture and a reinforced epitendinous suture but in a splint with the thumb position altered and the fingers also splinted. Other reports include those from Percival and Sykes,24 Noonan and Blair,25 Nunley et al,26 Fitoussi et al,28 and Kasashima et al.29 Most recently, Giesen et al31 published the latest results of repair of the FPL tendon. They analyzed 50 FPL tendon repairs using a six-strand core repair method, without peripheral sutures. Excellent or good results were recorded in 78% and 82% of cases (White and Buck-Gramcko criteria, respectively). No patients ruptured repairs as a result of early active mobilization. None developed tendon dehiscence postoperatively. The important message from this report is perhaps that a strong core suture can adequately tolerate early active tendon motion without the incorporation of peripheral sutures, which is a conceptual evolution in the treatment of flexor tendon injuries and may lead to significant simplification of surgery.
The case series presented by Elliot and his colleagues27,30,31 over the past 20 years reflects some unique findings relating to repair of FPL injury. Their outcomes were increasingly improved from a rupture rate of 17% to the present 0% rate. Their methods of tendon repair and rehabilitation evolved greatly. The thumb flexor tendon appears capable of returning to near-ideal function after proper repair and rehabilitation.
The use of stronger surgical repairs improved outcomes compared with the earlier reports using weaker repair methods but has not entirely eliminated postoperative repair rupture.20–22 It is the combination of strong surgical repair, proper venting of the pulleys, and early active motion, which reported recently,31,39,41 that has produced more consistently good or excellent outcomes without postoperative repair ruptures.
Over the past 20 years, the conceptual evolution in tendon repair has been remarkable and the technical innovations have been numerous. The most significant changes are (1) use of stronger surgical repairs (including core and peripheral sutures), (2) incorporation of a variety of early active motion regimens in postsurgical exercise, and (3) a redefinition of the management of the pulleys (see Chapters 9 and 10





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


