Chapter 39 Customizing Flexor Rehabilitation Based on Zone or Type of Injury
Outline
In recent years a significant amount of research in the field of flexor tendon treatment has contributed to advances in both surgical and rehabilitation techniques.1,2 There is an overwhelming amount of evidence to show that carefully devised rehabilitation programs are critical to achieving favorable outcomes following primary flexor tendon repair in the digits, but very little attention has been given to other zones of injury in the hand and forearm. Whatever the level of injury, the ultimate goal of both the surgeon and the therapist is to minimize or modify peritendinous adhesions and promote optimal tendon glide. At the same time the tendon repair must be protected from excessive stress to avoid gapping or rupture at the repair site.
Although early mobilization of primary flexor tendon repairs is now accepted practice, there is no one definitive rehabilitation regimen guaranteed to restore a full range of active digital motion. Therapists dealing with these injuries require not only specialized knowledge in the field but also the ability to use advanced clinical reasoning skills to select appropriate postoperative exercise programmes.3 Early active motion in different forms, used in conjunction with multistrand repair techniques, has gained increasing popularity but application must depend on consideration of a number of variables.1–3 The aim of this chapter is to examine the implications of these variables on regimen selection and assist the therapist with the provision of evidence-based practice following primary flexor tendon repair at all levels.
Extent of Injury
Injuries to the Skin
The nature of the skin wounds affects the decision making during rehabilitation. Untidy wounds, including a crushing element, will impact the final outcome and the therapist must prioritize the prevention of joint and scar contracture. The therapist should differentiate between incisions made during the surgery and those that are part of the original injury. Carefully designed surgical incisions made to access the tendon for exploration and repair of the tendon and other structures will minimize postoperative contracture. Random longitudinal wounds which cross the metacarpophalangeal (MCP) and the interphalangeal (IP) joints may cause joint contracture.4 When the surgical incision is made across these joints, active digital extension exercises and prophylactic splinting should be incorporated into the regimen to prevent loss of full joint extension.2–4
In more severe soft tissue injuries, the presence of skin grafts or flaps necessary for wound closure delays the start of postoperative mobilization until vascularity is ensured. In digital-level injuries, care must be taken not to impede joint motion or increase resistance to tendon glide by the use of restrictive dressing. Dressings should be shaped to reduce the resistance over the IP joints and should cover the wound area only, avoiding the use of circumferential adhesive tape (Figure 39-1). Postoperative complications such as infection, heavily exuding wounds or skin loss may require more substantive dressings, which will result in delays in initiating active motion. In cases where there is infection involving the tendon sheath, all motion should be delayed until the infection is treated. Where the status of the wound has the potential to impede active motion, for example, in large open wounds with extensive edema, mobilization must be confined to gentle passive exercises to preserve tendon glide and minimize stress on the repair until the restrictive swelling has reduced. In the presence of heavily exuding wounds, dressings should be removed on attendance for hand therapy, and provided there is minimal edema, a controlled active motion regimen may be initiated even in the presence of skin loss.

Injuries to Bone and Joint
Concomitant injuries to bone impact postoperative management as the timing and type of exercises chosen can be limited by the presence and characteristics of the bony injury and the stability of fracture fixation. Primary tendon repair is contraindicated in the presence of complex unstable or intra-articular fractures.2 In the case of stable, undisplaced fractures in the hand or digits, it is possible to initiate an early motion regimen, providing supplementary splinting support for the fracture while at rest and additional manual support when performing exercises. Rigid fixation of fractures of the phalanges or metacarpals usually provides sufficient stability to permit the early passive and active motion following discussion with the surgeon regarding safety. Injuries to more than one digit presenting with different patterns of injury in each require individual exercise plans for each digit. Care must be taken, however, initiating an active motion protocol in complex injuries to the middle, ring, and little fingers due to the quadriga effect of the conjoined flexor digitorum profundus (FDP) tendons. The most severely injured digit will dictate the mobilization program and the therapist must devise an exercise regimen that most effectively preserves the tendon glide for each digit without placing excessive stress on the repairs. This will be a combination of passive only exercises for the more seriously injured digits and careful active for those able to withstand greater stress. In the presence of joint stiffness, restoration of passive motion of the joint is imperative. Deep lacerations to the digits may damage the palmar plate or capsule of the IP joints, resulting in flexion contracture of the joints. Prophylactic extension splinting is indicated to prevent the contracture from the early stages of rehabilitation.
Vascularity of Injured Structures
Injuries requiring revascularization (e.g., digital replantation) require careful management. Early mobilization regimens should not be initiated until the viability of the digit is established. Whether damage to the vincula affects adhesion formation remains uncertain.5
Type of Tendon Injury
Complete or Partial Injuries
Complete divisions of tendon require protected mobilization and a customized program of exercises with no functional activity of the hand for at least 6 weeks. Less severe forms of the partial tendon injury (cut through less than 40% of the cross section) can be managed conservatively without surgery. The patients should be permitted to move their injured fingers without restrictions.7 Surgically repaired partial lacerations of the tendon (cut through greater than 40% of the cross section) are usually capable of withstanding the stresses of an active motion protocol and are less likely to rupture. The hand requires some form of dorsal splint protection but this may be removed as early as 3 to 4 weeks.
Flexor Pollicis Longus (FPL) Injury
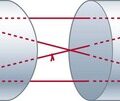
The postoperative care of the repaired FPL tendon requires special consideration. The FPL tendon appears to have a greater tendency to rupture when active motion regimens are applied following a two-strand core suture with simple peripheral stitches.8,9 Recent studies support the use of active motion programs following a multistrand core, even without an epitendinous suture.10,11 If there is any doubt as to the ability of the repair to withstand active motion the therapist should use passive motion techniques. When using a controlled active motion regimen, care must be taken to ensure that movement is isolated to the IP joint (Figure 39-2). A neutral position at the wrist benefits both flexion and extension at the IP joint. Positioning the wrist in extension can impede active extension at the IP joint and place stress on the repair site.

Other Factors
The Type and Quality of the Repair
There has been a significant amount of research devoted to improving the tensile strength of flexor tendon repairs, permitting greater confidence in the use of active mobilization regimens and resulting in reduced rates of dehiscence.12–14 Although some have demonstrated the successful application of active mobilization regimen with two-strand repairs of varying techniques, others have reported unacceptably high rates of rupture.15–17
Before selecting an appropriate postoperative regimen the therapist should be acquainted with the caliber and type of both core and circumferential suture in each particular case. Four- or six-strand core suture repairs with 4-0 or 3-0 suture produce a repair strong enough to accommodate early active motion of the repaired digital flexor tendon. If the tensile strength of the repair is judged not to withstand the forces generated during active digital motion, alternative and safer methods of maintaining tendon glide should be considered.18,19 Venting the constrictive part of a major pulley (such as the A2) will decrease the resistance to the tendon. Repairing the tendon just distal to the A2 pulley, without venting the constrictive part of the pulley, may subject the tendon to greater resistance during early active tendon movement. Particular care should be taken when instructing the patient to move the tendons that are repaired just distal to the A2 pulley, as greater incidence of rupture of the primary repair is experienced in this area.
Patient Characteristics and Compliance
The ability to comply with a rehabilitation regimen, which involves commitment to a strict exercise program within a protective splint for several weeks, vary among individuals. Age, medical and mental health, and socioeconomic factors influence the choice of postoperative management. Repairs are at risk of rupture if the patient removes the splint for function and of poor gliding action if they do not perform the required exercises. Enhancing compliance requires a confident, knowledgeable, and enthusiastic therapist who develops a good working relationship with the patient. Good communication, the provision of high quality information, and the enlistment of family support are also necessary. A regimen that is versatile and tailored to suit the lifestyle, socioeconomic circumstances, and work commitments of the patient also promotes cooperation. Negative factors that are most likely to impact on compliance and lead to poor outcomes are long travel distances to therapy and long waiting times. Postoperative pain, especially that which is neurogenic in origin, should be effectively controlled as this will significantly affect compliance and behavior.20,21 Despite the best efforts, the therapist is often presented with patients who do not or are unable to adhere strictly to the requirements of the rehabilitation regimen for a variety of reasons. In these situations a compromise must be reached to prevent repair rupture while permitting the patient to continue with certain aspects of their daily life.
Age
The choice of immediate aftercare following tendon repairs in children depends solely on the maturity of the child. The principles of postoperative management are similar to those applied to adults but the ability to comply with splinting and exercises must be carefully considered. Older children and teenagers will be able to follow a specific regimen, but younger children may inadvertently use the hand in functional activity and a splint guard is thus required to deter use of the injured hand (Figure 39-3). Although younger children may cooperate with a thermoplastic splint and a guard, they will require assistance with mobilizing exercises and the responsibility for this then falls to the carer. The selection of the type of exercises then depends on the capability of the carer and their ability to comply. Babies and toddlers are at risk of dehiscence through falls and functional activity and cannot follow mobilization regimens. For this reason the hand should be immobilized in a substantial, occlusive dressing for a period of 4 weeks. An effective way to protect the tendon repairs is the application of an above elbow plaster of Paris or resin cast. Nevertheless, both are prone to slippage and may require removal under anesthesia in some children. In our experience, a well-padded, occlusive, boxing glove–type dressing using generous amounts of adhesive tape to prevent removal is equally effective (Figure 39-4). This type of dressing can be easily reapplied in an outpatient setting during the 4-week period of immobilization, permitting inspection of the wound and integrity of the repair along with passive exercises. The paucity of literature on the subject leaves the therapist with little guidance in this field. Much depends on the ability of the child to cooperate with a regimen likely to provide the most optimal outcome. Immobilization for 4 weeks in the very young child has no detrimental effects on the result.22

Zone of Injury