This study used stromal vascular fraction gel (SVF-gel), a mechanically processed fat-derived product, to treat eye bag and tear trough deformity. SVF-gel is prepared by a process of centrifugation and intersyringe shifting and is particularly rich in SVF cells and native adipose extracellular matrix. SVF-gel injection is used alone or combined with transconjunctival eye bag removal. High satisfaction was noted among patients treated with SVF-gel injection for periorbital rejuvenation with fairly low complication rates. SVF-gel injection is a good alternative to assist transconjunctival lower eyelid blepharoplasty and correct the palpebromalar groove, tear trough deformity, and supraorbital hollow.
Key points
- •
The preferred donor sites for facial fat grafting are the abdomen or thigh.
- •
Stromal vascular fraction gel (SVF-gel) is prepared by a series of mechanical processes, including centrifugation and intersyringe shifting.
- •
SVF-gel is particularly rich in SVF cells and native adipose extracellular matrix (ECM).
- •
SVF-gel injection shows greater therapeutic effect in correcting the palpebromalar groove, tear trough deformity, and periorbital hollow.
Video content accompanies this article at http://www.plasticsurgery.theclinics.com .
Introduction
Aesthetic changes of the lower eyelid and midface represent some of the earliest clinically detectable areas of aging on the face. During the aging process, the supporting ligaments and tissues of the face and eyes experience irreversible changes, which combine to create a vertically elongated lower eyelid, a lax lower eyelid and protrusion of orbital fat, and ptotic malar/cheek complex. To eliminate the “tired appearance,” the surgeon attempts to reverse aging and gravitational changes in the lid/cheek complex with a goal to shorten that distance and suspend tissues.
For several years, the traditional surgical approach to lower eyelid blepharoplasty was to remove the pseudoherniated orbital fat via a transconjunctival or transcutaneous incision. The transconjunctival lower eyelid blepharoplasty offers an advantageous access to the lower eyelid and midcheek with no trauma to the anterior lamella of the lower eyelid and its quick recovery. However, infraorbital sunken and skeletal appearance of the eye was easily created when excessive orbital fat was excised. Additionally, conventional excision of excess intraorbital fat cannot sufficiently correct contour irregularities and attenuate tear trough deformity.
To avoid infraorbital hollow, fat repositioning techniques or filling techniques using autologous or nonautologous materials are increasingly applied. , The advantage of autologous fat grafting to the infraorbital area is achieving midcheek augmentation and improving the palpebromalar groove and addressing the tear trough deformity without disrupting the middle lamellae. However, traditional fat grafting is not an optimal alternative for periorbital injection because it uses particles of fairly large size, which may easily result in uneven skin surface or excess fullness.
In this article, we reported a novel adipose tissue–derived product called stromal vascular fraction gel (SVF-gel) for the purpose of infraorbital injection to correct infraorbital hollow and tear trough. SVF-gel is prepared by a process of centrifugation and intersyringe shifting. It has a smooth texture and is injected though a fine, 27-gauge needle. SVF-gel is particularly rich in SVF cells and native adipose extracellular matrix (ECM). SVF-gel can thus act as a natural filler, because it contains condensed adipose tissue ECM fibers. To validate its promising clinical applications, several case examples are presented to highlight those well-designed steps in fat grafting for facial rejuvenation, especially for the periorbital area.
Preoperative evaluation and special considerations
Each patient’s general health conditions and past medical or surgical history should be reviewed first. The major exclusion criteria includes a history of trauma or other comorbidities, operation, or filler injection in the injection area. Three-dimensional photographs are routinely taken and recorded before the surgical procedure and the individual aging degree especially the gravitational changes in the lid/cheek complex should be carefully evaluated and noted. Because the quality of facial skin and facial anatomy varies from person to person, signs of facial aging, such as soft tissue atrophy, structural ptosis, laxity of skin, and abruptly emerging lines, are analyzed and documented with detail. The potential donor sites for fat grafts harvested should also be carefully examined and marked.
Harvest of fat grafts should be performed under general anesthesia. The tumescent solution used for donor site analgesia and hemostasis should contain the lowest concentration of lidocaine and ropivacaine because their high concentration has been proved to impair the adipocyte function. In general, we use 0.03% of lidocaine and 0.01% of ropivacaine in 500 mL of normal saline. The tumescent solution also contains epinephrine with a concentration of 1:100,000. Epinephrine can precipitate vasoconstriction in the donor sites, which tends to decrease the quantity of blood loss, occurrence of bruising and hematoma, and the possibility of intra-arterial injection of the transplanted fat particles especially when injecting around periorbital or temporal area.
Because SVF-gel is rich in SVF cells and native adipose ECM and the oil drops have been massively wiped off through a process of centrifugation and intersyringe shifting, SVF-gel manifests an obviously higher retention rate than traditionally processed fat grafts after transplantation. The injection volume of SVF-gel mainly depends on the volume depletion of soft tissue based on the preoperative evaluation. Unlike traditional fat grafting, because SVF-gel has a great retention rate of 80%, overcorrection is not necessary in SVF-gel injection.
Surgical procedures
Donor Site Selection
In clinical practice, lower abdomen and inner thigh are the optimal donor sites for fat graft harvest because well-designed suction in these sites could significantly enhance the body contour and they are accessible in the supine position in which facial rejuvenation is performed. Besides, fat reserves in lower abdomen and inner thigh are adequate for the production of SVF-gel. According to published literature, fat grafts harvested from lower abdomen and inner thigh are reported to have higher concentration of adipose-derived stem cells. Thus we routinely choose lower abdomen and inner thigh as the donor sites.
Fat Graft Harvesting
After local anesthesia, incisions should be done in the specified locations where the scar is easily concealed. Usually lower abdomen and inner thigh incisions are symmetric and located on the margin of pubic hair and on the groin, respectively, with the size of 5 to 10 mm. A cylindrical clamp is sutured to the skin to reduce the mechanical trauma during the process of liposuction and to dilate the underlying subcutaneous tissues through the incision to allow insertion of the harvesting cannula. The tumescent solution is then equably infiltrated to the donor sites 10 minutes before fat extraction, which makes harvesting of fat grafts easier to operate with less trauma and makes the patient less painful in the recovery. It should be noted that the tip of the infiltration cannula we specially designed is usually blunt and has multiple oblong openings on the side. Usually a 20-mL Luer-Lok syringe is connected with a harvesting cannula with a 2.5-mm inner diameter for liposuction. This kind of cannula is more efficient for fat extraction. Gentle pulling back on the plunger creates a space vacuum negative pressure in the syringe. With gentle back and forth movement of the assembled syringe, the fat is gradually collected. After harvest, all incision sites are closed with interrupted sutures once excess tumescent fluid is milked out.
Fat Graft Processing
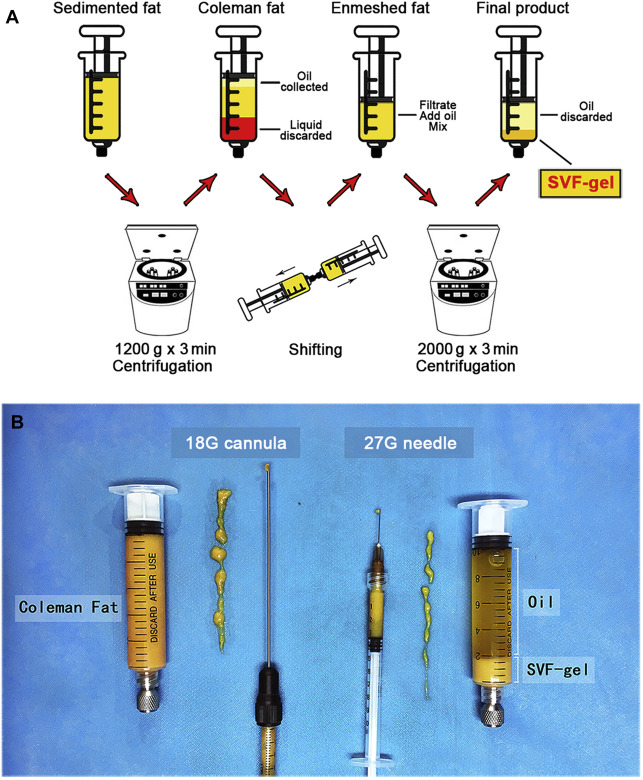
SVF-gel was obtained as previously reported ( [CR] ). Standard Coleman fat was the product we use to make SVF-gel. The Coleman fat was prepared according to the standard Coleman technique. The lipoaspirate was centrifuged at 1200 × g for 3 minutes to obtain Coleman fat in the middle layer. The bottom layer of the tumescent fluid was discarded, and 20 mL of Coleman fat was transferred to two 20-mL syringes connected by a Luer-Lok connector (internal diameter of 1.4 mm). The Coleman fat was then transferred between two syringes (six to eight times) at a rate of 20 mL/s until the Coleman fat converted into a uniform emulsion, which was then centrifuged at 2000 × g for 3 minutes. The middle layer, which had a volume of approximately 20% of the original Coleman fat, was identified as SVF-gel and collected for further use ( Fig. 1 ).
Related posts:
 Facial Fat Grafting
Facial Fat Grafting
 An Overview of Principles and New Techniques for Facial Fat Grafting
An Overview of Principles and New Techniques for Facial Fat Grafting
 Fat Grafting for Facial Contouring (Temporal Region and Midface)
Fat Grafting for Facial Contouring (Temporal Region and Midface)
 Fat Grafting for Facial Contouring (Nose and Chin)
Fat Grafting for Facial Contouring (Nose and Chin)
 Fat Grafting for Treatment of Secondary Facial Deformity
Fat Grafting for Treatment of Secondary Facial Deformity
 Prevention and Management of Serious Complications After Facial Fat Grafting
Prevention and Management of Serious Complications After Facial Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


