Fat grafting has evolved over the past two centuries and has revolutionized regenerative medicine, aesthetic and reconstructive surgery. Fat grafting provides a safe and minimally invasive technique to improve signs of aging, sun damage, and congenital and acquired craniofacial deformities. The Coleman technique for harvesting, processing, and grafting provides a reliable strategy for consistent results. However, unanswered questions remain regarding the biology of fat grafting, survival mechanisms, and regenerative properties. The future of fat grafting is bright and includes cell-based therapy and extracellular matrix–based scaffolds. This article provides an overview of the past, present, and future of facial fat grafting.
Key points
- •
Fat grafting has revolutionized regenerative medicine, aesthetic and reconstructive surgery.
- •
Fat grafting provides a safe and minimally invasive technique to improve signs of aging, sun damage, and congenital and acquired craniofacial deformities.
- •
The Coleman technique for harvesting, processing, and grafting provides a reliable strategy for consistent results.
- •
Many unanswered questions remain in terms of the biology of fat grafting, survival mechanisms, and regenerative properties.
- •
The future of fat grafting includes cell-based therapy and extracellular matrix–based scaffolds.
The past
The history of facial fat grafting represents a tortuous path in search of a minimally invasive alternative to solve simple and complex soft tissue defects. It is through reflection, criticism, and determination that over the past two centuries fat grafting has gone from being a challenging surgical technique to a beacon of hope for aesthetics, reconstructive surgery, and regenerative medicine.
Fat grafting was first described in 1893 by the German surgeon Gustav Neuber, who transplanted adipose tissue from the arm to the lower orbit to correct unsightly, depressed, and adherent scars caused by osteomyelitis. Although he reported good results, he encountered considerable resorption rates. In 1895, another German surgeon Vincent Czerny described transferring a fist-sized lipoma from the buttock to the breast to improve symmetry following unilateral partial mastectomy for fibrocystic mastitis. In 1910 and 1912, Eugene Holländer reported injections to the face of human fat mixed with ram fat heated to body temperature to correct facial lipoatrophy. He also advocates that should the skin be adherent as occurs in trauma or in bony diseases, the scar between the bone and the skin should be released. The German maxillofacial surgeon Erich Lexer used fat and local flaps and cartilage graft to reconstruct the eye socket to accommodate a prosthesis. He subsequently published in 1919 a two-volume book that devoted 300 pages to fat grafting. He described the use of fat grafting for treatment of various pathologies including the treatment facial trauma sequelae, hemifacial microsomia, and treatment of knee ankylosis and tenolysis with fat grafting. This is proof that the reparative and regenerative aspects of fat grafting have been recognized for almost a century. Plastic surgery pioneer Sir Harold Gillies also described in 1920 the use of fat parcels for the reconstruction of various facial wounds with good results. The initial enthusiasm for en-bloc fat transplantation slowed down because of the increasing evidence of fat reabsorption and oil cyst formation, which led to unreliable, hard, and fibrotic tissue. So other facial fillers were attempted through the years including paraffin, silicone, gutta-percha, celluloid, or rubber sponges. Charles C. Miller was one of the first US cosmetic surgeons to use some of these products to correct facial defects, such as crow’s feet and nasolabial folds. He also described the use of a piece of adipose tissue harvested from the abdomen and reinjected in facial defects using a special screw piston syringe. However, the use of adipose tissue as injectable did not catch traction until the introduction of liposuction in the 1980s with Pierre Fournier and Yves Gerard Illouz. The adoption of cannulas to remove adipose tissue with a minimally invasive technique was a game changer not only for body contouring but also for the evolution of fat grafting. This allowed reinjection of a more liquid form of fat instead of reinsertion of en-bloc adipose tissue. Despite the innovative harvesting technique, almost complete reabsorption of the fat graft persisted. For this reason, a more systematic approach of harvesting was needed to optimize fat grafting survival, aesthetic outcomes, and minimize donor site morbidity. In 1994, SRC published the technique that would revolutionize the modern aesthetic and reconstructive surgery and open the doors to regenerative medicine.
The present
The Coleman technique has been popularized by Coleman since mid-1990s and has been considered, at least by most surgeons, a standardized technique for facial fat grafting. The original technique involved harvesting, purification, and injection with the goal of separating out the unwanted components (oil, blood, local anesthetic, and other noncellular material) through centrifugation and injecting the fat in tiny aliquots with each pass of the cannula. Since its original inception the technique has been refined and improved.
Indications for Facial Fat Grafting
Indications for fat grafting to the face include aging changes, sun damage, and soft tissue deformities. Rhytids are smoothed with intradermal and superficial fat grafting. Orbital and temple hollowing are improved with fat grafting. Volume deficiency (eg, lips) is restored by augmentation. Fat grafting can improve definition of jawline and zygomatic region. Fat grafting can also be used for congenital and acquired soft tissue deformities, such as Parry-Romberg syndrome, craniofacial microsomia, Treacher Collins syndrome, human immunodeficiency virus–related lipodystrophy, scarring, surgical defects, and traumatic soft tissue loss.
Harvesting
Depending on patient preference and the volume of fat required, fat is harvested under either local or general anesthesia. For straight local cases, nerve blocks may be performed. The infiltration solution consists of 0.5% lidocaine with 1:200,000 epinephrine buffered with sodium bicarbonate (or diluted to half the strength to provide a larger volume) infused with a Lamis (or other blunt) infiltration cannula (Mentor Worldwide LLC, Santa Barbara, CA). When intravenous sedation or general anesthesia is required for harvests of larger volumes of fat, the infiltration solution of choice is 0.1% lidocaine with 1:400,000 epinephrine. For either case, the volume of tumescent solution infused should usually be less than the amount of fat to be harvested. A multihole Coleman harvesting cannula attached to a 10-mL syringe is then used to suction the fat. The two-hole cannula originally described in the 1994 paper was replaced by a multihole cannula because of safety concerns because the two-hole cannula would constantly clog and was a safety hazard if dealing with patients with blood infectious diseases. The plunger of the syringe is pulled back only a few milliliters to create enough negative pressure to harvest the fat, while avoiding excessive pressure that could rupture fat cells. On completion of the fat harvest, the incisions are closed with interrupted sutures.
Transfer and Purification
After each 10-mL syringe is filled, the cannula is disconnected, a Luer-Lok cap (Becton, Dickinson and Company, Franklin Lakes, NJ) is placed, and the plunger is removed. Syringes are then placed in a sterilized centrifuge rotor and spun at 1286 g for 2 minutes to separate the components of the tissue. The original description of centrifugation at 3400 rpm was replaced by a more accurate gravitational measure because of its increased accuracy (rpm does not take into account the radius of the centrifuge). The centrifugation process concentrates growth factors and stromal vascular fraction (SVF). The oil on the surface is decanted, and the Luer-Lok cap is then removed, allowing the aqueous layer to be drained from the bottom of the syringe. A Codman neuropad (Codman Neuro, Raynham, MA) or Telfa strip (Telfa Strip, Salem, MA) is then placed in the top of the syringe to wick away the remaining oil. The processed fat is then transferred to 1-mL syringes for placement. Centrifugation results in graded densities of the fat, and the highest-density fat remains at the bottom of the 10-mL syringes. Studies have shown better graft take for high-density fat compared with low-density fat. Therefore, when transferring fat from the 10-mL to 1-mL syringes, the injection syringes should be grouped into high-density, intermediate-density, and low-density groups to allow for more thoughtful placement. SRC transitioned from 3-mL to 1-mL syringes because of improved tactile and quantity accuracy in fat delivery.
Infiltration
Incision sites are anesthetized with 0.5% lidocaine with 1:200,000 epinephrine before making stab incisions with a No. 11 blade. A small volume of 0.5% lidocaine with 1:200,000 epinephrine is then infused into graft sites for anesthesia and vasoconstriction. Vasoconstriction reduces the risk of inadvertent intravascular infusion and reduces postoperative bruising. Decanted oil collected during the fat processing stage is used when available to lubricate the incision sites during harvesting to avoid friction on the puncture or incision sites. One of the keys to the success of the Coleman technique is placing the parcels of grafted fat in proximity to an adequate blood supply. To create this environment, fat should be placed in small aliquots surrounded by native tissue. These aliquots should be placed as the microcannula is withdrawn, and no more than 0.1 mL of fat should be placed with each pass. The initial small 17-gauge cannula has been replaced for even smaller ones specifically in facial fat grafting to improve the accuracy of the delivery and because transferring fat parcels that are too large results in fat necrosis, fat resorption, oil cysts, or irregularities. The presence of scar should be addressed by releasing any adhesions using an 18-gauge needle, V or W dissector perpendicularly, and then injecting an appropriate volume of fat into that area. Different depths of fat placement should be used, depending on the desired effect. Fat placed in the intradermal or subdermal layers is ideal to improve wrinkles, and the overall complexion and skin quality. However, at this level, care should be taken to avoid damaging the subdermal plexus and creating superficial irregularities. Fat placed deep against the periosteum is used to change how the remaining soft tissue envelope drapes over the bony structure of the face. Fat placed in the intermediate subcutaneous layers restores volume to rejuvenate or establish a different facial proportion. Molding of the fat placed at any level should be avoided, because this may lead to fat necrosis and resorption. On completion of graft placement, infusion sites are closed with interrupted sutures. A small volume of concentrated fat (approximately 0.2–0.3 mL) is then placed into the closed incisions using a 22-gauge needle; this is done to aid in healing of the incisions. Standard postoperative liposuction garments or compressive dressings are applied to the donor sites to prevent hematoma and seroma formation. For the first 72 hours postoperatively, cool (but not ice-cold) compresses may be applied to the face intermittently to reduce discomfort, bruising, and swelling. Various dressings were initially trialed but most were cumbersome and no benefit was noticed. Thus, facial dressings were abandoned all together. Deep massage of the face should be avoided, because it can cause fat migration or necrosis. However, light touch is performed to encourage lymphatic migration.
Case Demonstration
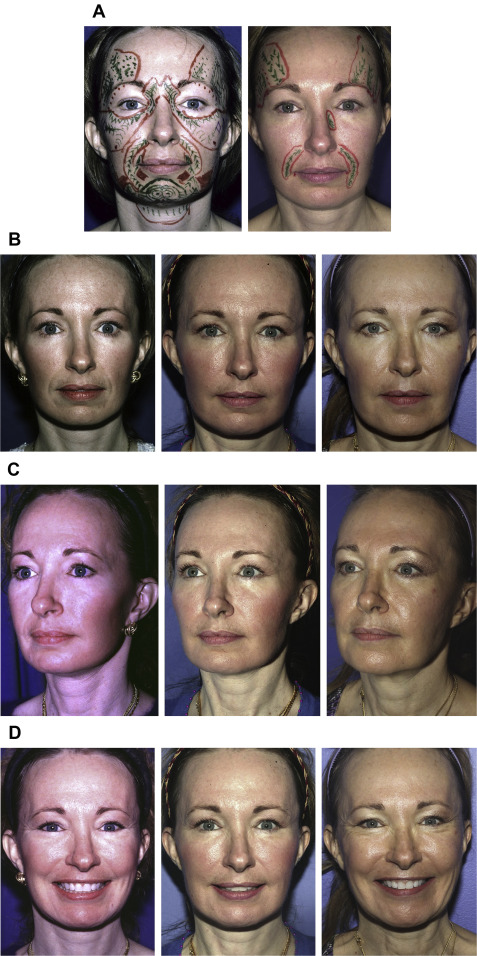
A 44-year-old woman with a past medical history of face-lift and lower and upper lid blepharoplasty presented with hollowing of the orbits, tear troughs, deepening of her nasolabial folds, loss of malar prominence, perioral rhytids, marionette lines, and loss of definition of her jawline. A total of 200 mL fat was harvested from her thighs and knees and processed using the Coleman technique. Fat was grafted in the right temple (6 mL), left temple (6 mL), glabella (1.5 mL), right medial eyelid (0.5 mL), left medial eyelid (0.5 mL), right anterior malar fold (1.5 mL), left anterior malar fold (1.5 mL), right anterior malar region (3 mL), left anterior malar region (4 mL), right lateral malar region (7 mL), left lateral malar region (8 mL), right nasolabial fold (7 mL), left nasolabial fold (5 mL), right buccal cheek (6 mL), left buccal cheek (4 mL), right mandibular jawline (4 mL), left mandibular jawline (4 mL), mental groove (0.5 mL), and submental region (6 mL). Two years later the patient was pleased with the result but desired minor enhancements. A total volume of 40 mL was harvested and grafted in the right temple (4.7 mL), left temple (3.5 mL), left side of her nose (0.6 mL), right nasolabial fold (1 mL), and left nasolabial fold (3 mL). Preoperative and 10-year postoperative photographs are shown in Fig. 1 . The patient has a lasting volume restoration and skin quality improvement.
Related posts:
 An Overview of Principles and New Techniques for Facial Fat Grafting
An Overview of Principles and New Techniques for Facial Fat Grafting
 Fat Grafting for Facial Rejuvenation through Injectable Tissue Replacement and Regeneration
Fat Grafting for Facial Rejuvenation through Injectable Tissue Replacement and Regeneration
 Fat Grafting for Facial Contouring (Temporal Region and Midface)
Fat Grafting for Facial Contouring (Temporal Region and Midface)
 Fat Grafting for Facial Contouring (Nose and Chin)
Fat Grafting for Facial Contouring (Nose and Chin)
 Fat Grafting for Treatment of Secondary Facial Deformity
Fat Grafting for Treatment of Secondary Facial Deformity
 Prevention and Management of Serious Complications After Facial Fat Grafting
Prevention and Management of Serious Complications After Facial Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


