The concept of microautologous fat transplantation (MAFT), proposed by Lin and colleagues in 2007, emphasized that the volume of each delivered parcel should be less than 0.01 mL to avoid potential fat grafting morbidities. The MAFT-GUN facilitates control of the parcel volume and therefore substantially avoids central necrosis and associated complications. In this article, the authors present a simple, reliable, and consistent procedure based on MAFT for profiloplasty. Favorable outcomes with sustainable long-term effectiveness were obtained, further confirming that the MAFT technique is an alternative for facial contouring in the nose and chin.
Key points
- •
Microautologous fat transplantation (MAFT) has been postulated by the primary author, who have demonstrated its efficacy using the MAFT-GUN.
- •
The indispensability of MAFT in facial applications has been shown for sunken upper eyelid, temple and forehead recontouring, primary augmentation rhinoplasty, and gummy smile correction.
- •
The technique for Asian profiloplasty, using MAFT on the nasal dorsum and chin areas, has shown a favorable aesthetic result.
Video content accompanies this article at http://www.plasticsurgery.theclinics.com .
Introduction
In 1963, Dr Landazuri was the first surgeon to use the term “profiloplasty,” defined as rhinoplasty plus mentoplasty. Asians often look to enhance the appearance of the nasal dorsum and chin profile due to certain ethnic deficiencies. Various nasal and chin implants have been adopted for this purpose. However, the results seemed unsatisfactory and potential morbidities were often bothersome. In past decades, fillers have garnered attention, despite complications and other concerns such allergy, necessity of repeat injection, and the cost-effectiveness.
Fat grafting was first described by Neuber in 1893 and continues to be performed frequently because of the ease of fat harvest, abundance of graft material, and the lack of transplant rejection. However, fat survival and retention rates are unpredictable, and complications such as abscesses, cysts, nodulation, and neurovascular injury may occur.
Microautologous fat transplantation (MAFT) has been postulated by Lin and colleagues, and its efficacy has been demonstrated using the innovative instrument, MAFT-GUN to illustrate the indispensability in clinical applications for facial and body contouring and rejuvenation. In this article, the authors further demonstrate the technique for Asian profiloplasty of the nasal dorsum and chin areas to achieve favorable aesthetic appearance.
Preoperative evaluation and special considerations
Preoperative evaluation included previous operative history and existing sequelae due to any filler injection. The best candidates for MAFT in these areas are patients without history of surgery (synthetic implant or autologous/allogenic cartilage or bone graft) or filler injections. Nevertheless, MAFT might be considered in selected cases due to unavoidable previous procedures.
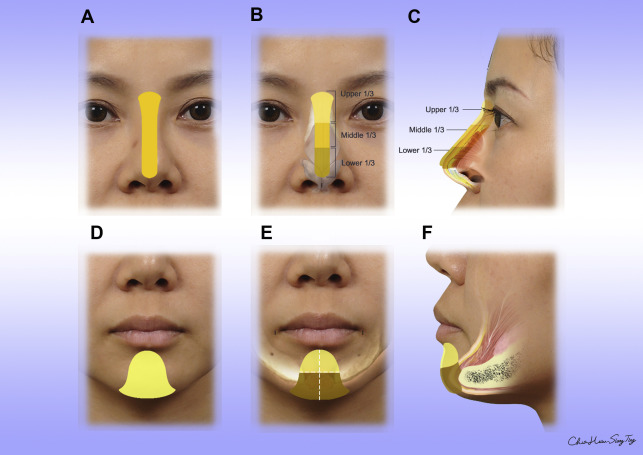
Preoperative markings were made with the patient seated. In the nasal dorsum, the recipient area for fat transfer was drawn in the shape of an I (width, 6–8 mm) from the nasal tip to a point approximately 15 mm above the intercanthal line ( Fig. 1 A) with a fan-shaped cephalic end. This pattern was further divided into upper, middle, and lower zones ( Fig. 1 B). In the chin area, a bell shape was designed centrally from the margin of the chin to 5 mm above the mentolabial sulcus ( Fig. 1 D) that was further symmetrically divided into upper/lower, right/left portions ( Fig. 1 E). The recipient areas were multiple layers from deep, middle to superficial layers ( Fig. 1 C, F).
Surgical procedure
All patients received total intravenous anesthesia before fat grafting. Appropriate local anesthesia was applied at donor and recipient inserting sites with 0.3 to 0.5 mL of 2% lidocaine HCl with epinephrine (1:50,000). Lipoaspirates were harvested from the lower abdomen or inner thigh where the adipocyte viability was greater. The donor site was infiltrated with a tumescent solution (10 mL of 2% lidocaine [20 mg/mL]: 30 mL of Ringer lactate solution: 0.2 mL of epinephrine [1:1000]). Approximately 10 to 15 minutes after infiltration, fat was harvested from the donor site with a blunt-tip cannula (diameter, 2.5 or 3.0 mm; ≥1 holes sized 1 mm × 2 mm). The lipoaspirate volume was approximately equal to the volume of the tumescent solution to ensure that fat constituted a major proportion of the lipoaspirate. To minimize damage to the lipoaspirate, the plunger of a 10-mL syringe connected to a liposuction cannula was withdrawn to approximately 2 to 3 mL to maintain a negative pressure of 270 to 330 mm Hg. Lipoaspirates were processed and purified by centrifugation at 3000 rpm (approximately 1200 g) for 3 minutes as described by Coleman. This procedure minimized graft contamination due to environmental exposure and manual manipulation. Centrifugation facilitated separation of the lipoaspirate into layers. The top layer contained oil from ruptured fat cells; the middle layer contained purified fat; and the bottom layer contained blood, cellular debris, and fluid. The purified fat was carefully transferred into a 1-mL Luer-slip syringe using a transducer. The syringe containing purified fat was loaded into a MAFT-GUN ( Fig. 2 ) and connected to an 18-gauge, blunt-tip cannula. The device was set by adjusting a dial to deliver fat parcels of 0.0067 mL (ie, 1/150 mL) to 0.0083 mL (ie, 1/120 mL) with each trigger deployment (see Fig. 2 ). A puncture incision was made on the nasal tip/bilateral mouth angles with a no. 11 scalpel blade (see Fig. 1 B, E) as an insertion point.

Fat Grafting Injection
Microautologous fat transplantation to the nasal dorsum
The fat transplantation procedure to the nasal dorsum was performed by pulling the trigger while withdrawing the MAFT-GUN. Meticulously, the parcels were transplanted in 3 layers of the nasal dorsum from the deepest to the most superficial layers (ie, from the deep areolar plane to the vascular/fibromuscular plane to the subcutaneous areolar plane) (see Fig. 1 C). During MAFT, downward traction was applied to successive zones of the nose with the surgeon’s nondominant hand. First, traction was placed on the middle third of the nose while grafting the upper third. Next, traction was placed on the lower third of the nose (ie, the nasal tip) while grafting the middle third. Fat was transferred to the nasal tip last. The nasal dorsum is roughly divided by three (upper-, middle- and lower-third) as figure. The volume of fat grafting to be transplanted on nasal dorsum was roughly distributed on each third. However, the upper third was approximately 40-50% of the total volume. The insertion wound was subsequently closed with 1 suture (6-0, nonabsorbable) ( [CR] and [CR] ).
Microautologous fat transplantation to the chin
Anatomic multiple-layer (deep: supraperiosteal, middle: periosteal to mentalis muscle/intermentalis muscle, superficial: mentalis muscle to skin) transplantation was performed in the chin area according to surgical planning (see Fig. 1 E, light brown). For those who wished to reduce the sharpness of the mentolabial sulcus, MAFT was particularly emphasized to blend this sulcus for a pleasing obtuse appearance (see Fig. 1 E, yellow). Although in this sulcus, the multiple-layer transplantation was also applied from oral mucosa to skin. The average volume in this sulcus area was 1.0 to 2.0 mL (see Fig. 1 E, yellow) and the volume of the chin augmentation was 2.0 to 4.0 mL (see Fig. 1 E, light brown). The bilateral insertions were closed with 6-0 nonabsorable sutures ( [CR] and [CR] ).
Postoperative care
Massage was avoided postoperatively in the recipient area. The donor area was dressed with compressive garments and the recipient with adhesive paper tape to alleviate swelling. Routine postoperative care, oral antibiotics, and nonsteroidal antiinflammatory drugs were administered for 3 days or as needed. The suture placed at the insertion site was removed 2 to 3 days postoperatively, and the sutures placed at the donor site were removed 1 week postoperatively. Gentle lymphatic drain massage was suggested 7 days after surgery to relieve swelling. All patients received routine follow-up at an outpatient clinic at 1, 3, 6 months and even longer postoperatively. Photographs were taken at each visit for comparisons over time.
Expected outcome and management of complications
About 80% of patients in the authors’ series (more than 500 cases, recontouring for nasal dorsum/chin or combined) for profiloplasty by MAFT technique were satisfied with a single procedure. No infections, cyst formations, nodulations, irregularities, or any severe complications were reported.
Revision or subsequent procedures
Touchup MAFT might be performed 4 to 6 months after the first procedure for those who requested further enhancement of the contouring.
Case demonstrations
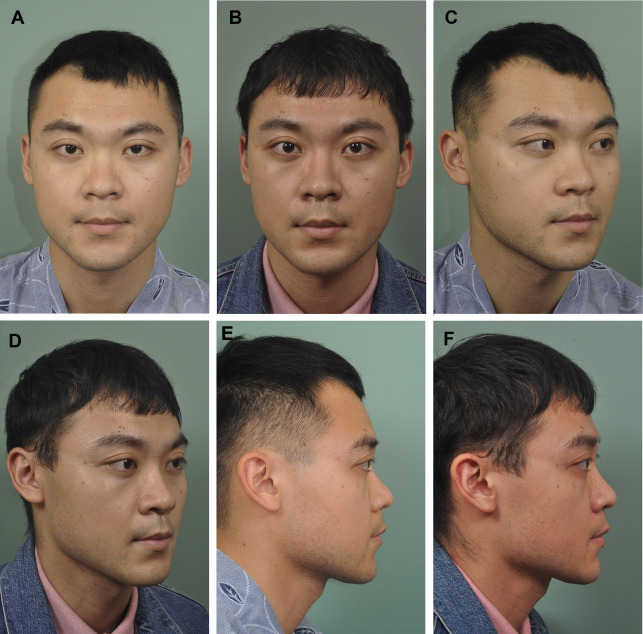
Case 1 . See Fig. 3 .
Related posts:
 Facial Fat Grafting
Facial Fat Grafting
 An Overview of Principles and New Techniques for Facial Fat Grafting
An Overview of Principles and New Techniques for Facial Fat Grafting
 Fat Grafting for Facial Rejuvenation Using Stromal Vascular Fraction Gel Injection
Fat Grafting for Facial Rejuvenation Using Stromal Vascular Fraction Gel Injection
 Fat Grafting for Facial Contouring (Temporal Region and Midface)
Fat Grafting for Facial Contouring (Temporal Region and Midface)
 Fat Grafting for Treatment of Secondary Facial Deformity
Fat Grafting for Treatment of Secondary Facial Deformity
 Prevention and Management of Serious Complications After Facial Fat Grafting
Prevention and Management of Serious Complications After Facial Fat Grafting
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


