Abstract
Severe central avulsive facial trauma injuries are typically not amenable to reconstruction using classical reconstructive techniques. Therefore, patients with these injuries are potential candidates for facial allotransplantation. In this chapter, a classification system for facial injuries that are amenable to transplantation is presented, in addition to descriptions of transplantation surgical techniques and postoperative management. Lastly, transplant-specific topics such as rejection and tolerance are discussed as they pertain to facial transplantation.
Keywords
vascularized composite allotransplantation, VCA, face transplantation, rejection, tolerance
Background
Facial Transplantation Experience
The first facial transplantation was completed in France in 2005. Since that time, over 37 facial transplantations have been performed around the world. Of these cases, at least 28 have been the result of facial trauma. In fact, most of these cases have been performed secondary to ballistic injuries (n = 15), burn injuries (n = 8), or animal attacks (n = 3). As the number of new vascularized composite allotransplantation (VCA) centers continues to expand across the globe, face transplantation has emerged as a viable treatment modality for the management of severely disfigured patients following facial trauma.
The early success of facial transplantation for severe facial disfigurements has addressed the difficulties often associated with complex facial trauma reconstruction. Facial trauma is associated with significant bony and soft tissue loss. In the case of ballistic injuries, extensive bony and soft tissue damage results from the kinetic injury dissipated by the impact of the bullet. Moreover, significant damage can occur due to the trajectory of the bullet. Unfortunately, the complexity of trauma-related injuries to the face makes the reconstructive effort difficult and often inadequate with conventional surgical techniques. Classically, reconstructive surgeons managed these injuries via multiple stages, often utilizing free tissue transfer reconstruction and other plastic surgery techniques. With immunosuppressive regimens now capable of achieving long-term allograft acceptance and current conventional reconstructive methods unable to achieve optimal facial aesthetic results, facial transplantation is now considered by some as a viable first-line treatment option in the patient with a central avulsive facial injury pattern.
Surgical Indications
Indications
Patient selection is the most important factor to consider before facial allotransplantation. The experience of the senior authors has revealed that proper evaluation and selection is the most important determinant of outcomes after facial allotransplantation. A multidisciplinary approach must be taken to not only assess the surgical indications for facial allotransplantation but also the psychological and social factors that may impact outcomes. These psychological and social factors are critical since postoperative rehabilitation, therapy, and correctional surgery are necessary postoperatively for optimal aesthetic and functional results.
Given that facial allotransplantation is still in its infancy, surgical indications for facial allotransplantation have yet to be fully established. Although this is a topic of great controversy, most reconstructive surgeons agree that patients with severe central avulsive facial trauma, with functional limitations (i.e., oral competence) not amenable to reconstruction using classical reconstructive techniques, should be considered as potential candidates for facial allotransplantation. Patients with central avulsive facial trauma meet this criterion, since they typically present with naso-orbital-ethmoid fractures, eyelid and nasal defects, anterior maxilla, palate, and mandible fractures, and defects of the upper/lower lips and tongue. This typical injury pattern, considered by some as “unreconstructable,” is completely addressed with facial allotransplantation in a single procedure. Traumatic burn injuries that result in extensive soft tissue loss of the lips and eyelids are also considered potential indications for facial allotransplantation ( Fig. 3.17.1 ).

Although absolute indications are still controversial, most reconstructive surgeons agree on the establishment of strict exclusion criteria. These criteria are established to reduce the risks associated with transplantation ( Box 3.17.1 ). For example, most agree that patients under the age of 18 should be excluded due to the difficulties of informed consent in this population. Additionally, patients over the age of 65 are generally excluded due to the known higher malignancy risk associated with immunosuppression therapy, although these are relative contraindications and not absolute.
| Age | Patients over 18 years and under 65 years |
| Vision | Although some centers believe that eyesight is important for functional recovery, many others do not believe blindness to be an absolute contraindication |
| Psychosocial assessment | Motivation for transplantation, social support system/family structure, emotional and cognitive preparedness, body image adaptation, history of medication compliance/substance abuse need to be evaluated |
Relative Indications
As the facial transplantation experience grows, improvements in immunoregulatory regimens may potentially increase the indications for facial allotransplantation to smaller defects. Currently, autologous reconstruction options for the oral commissure, nose, and periorbital complex are limited. The current standard of care for oral commissure reconstruction is hallmarked by oral incompetence. Furthermore, current techniques give the oral commissure an unnatural appearance, particularly when attempting to recreate the dry and wet mucosa. Similarly, few nasal reconstructive surgeons can achieve both satisfactory function and appearance for total nasal defects. Additionally, it is rare for large eyelid defects to result in functional protection and lubrication of the globe with a normal appearance. Given these shortcomings along with the success of transplanting these facial units as part of larger facial transplants, it is reasonable to predict superior outcomes transplanting these units in isolation compared to autologous reconstruction. With the risks of current lifelong immunosuppressive regimens, the benefits of such small facial unit transplantations need to be considered carefully in the context of the individual patient. Facial unit transplantation may be more conceivable at this stage in the setting of concurrent solid organ or other VCA from the same donor, as it would not significantly increase the potential morbidity of the procedure. Conversely, unit transplantation results in less morbidity if rejection requires explantation, and may allow for investigational immunotherapy trials with less risk posed in the event of rejection.
Classification
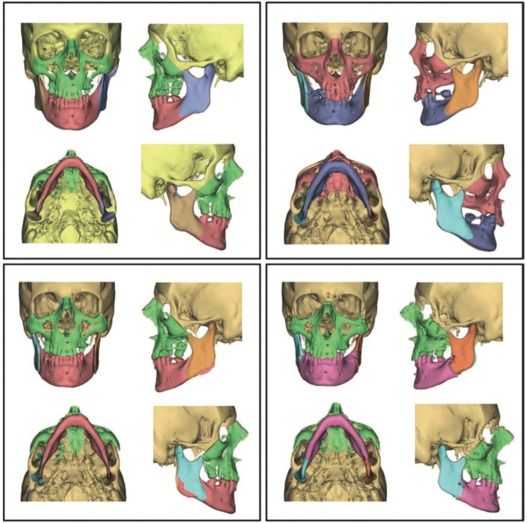
A classification system that accurately describes facial defects is necessary to: (A) document facial deformities; (B) develop treatment algorithms; and (C) develop indications for facial allotransplantation. The senior authors devised a working classification of facial allotransplants based on soft tissue functional–aesthetic subunits and the Le Fort classification for the craniofacial skeleton ( Fig. 3.17.2 ). Soft tissue defects were categorized into four zones ( Table 3.17.1 ) and bony defects were classified into four types ( Table 3.17.2 ). Based on this proposed classification, the senior authors believe that a predictable and modifiable treatment algorithm can be developed for the planning of facial allotransplantation. Although the application of this classification system is still in its infancy, we expect that future studies will examine its potential for advancing the field of facial allotransplantation.
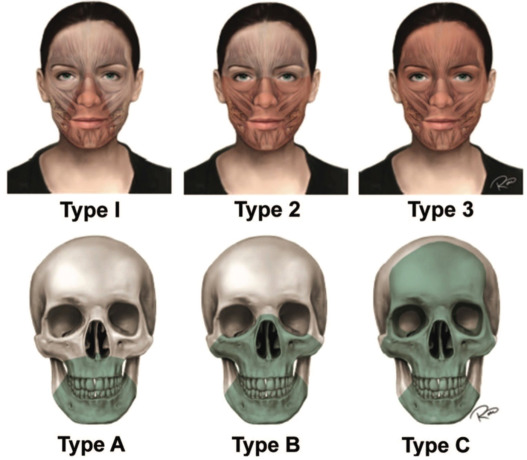
| Type | Functional Subunit | Anatomic Defects |
|---|---|---|
| 0 | Oral subunit | Upper lip, lower lip, and oral commissures |
| 1 | Oral–nasal subunit | Septum, nasal cartilage, and nasal soft tissues, with or without defects in type 0 |
| 2 | Oral–nasal–orbital subunit | Lower eyelids and malar soft tissues, with or without defects in type 1 |
| 3 | Full facial subunit | Palpebral and frontal regions, can include all soft tissues of the face |
| Type | Defect |
|---|---|
| M | Presence of mandibular defect |
| A | Maxillary alveolus (Le Fort I segment) |
| B | Nasal bones, maxilla, zygoma, vomer, ethmoid, inferomedial orbital bones, and defects in type 1 (Le Fort III segment) |
| C | Frontal bone, supraorbital rims, and defects in type 2 (Monobloc advancement segments) |
Surgical Techniques
Donor Procedure
Donor procurement has been extensively described by the senior authors in previous publications. In short, full facial allotransplantation is executed by sequential soft tissue and bony dissection. Before division of the pedicles, stereolithographic modeling can be used to tailor donor bony segments. This also allows for the pre-bending of plates before the beginning of ischemia time. After division of the pedicles, the allograft is taken to the back table where it is flushed with University of Wisconsin solution and then placed on ice.
Recipient Procedure
The recipient is brought to the adjacent donor operating room and the recipient dissection is started almost concurrently with the donor harvest procedure. This often requires a second team to minimize fatigue and optimize efficiency. Since most recipients have had multiple previous operations and extensive scarring from trauma, preparation of the recipient may take a long time (the first face transplant performed by the senior author required a recipient dissection time of 17 hours). Cutting guides and stereolithographic models can be utilized to optimize surgical efficiency ( Fig. 3.17.3 ).