Eyelid coupling using the modified tarsoconjunctival flap is an effective treatment for paralytic ectropion. Eyelid position and quality of life can be improved in patients with flaccid facial paralysis using these eyelid coupling procedures. The modified tarsoconjunctival flap can obscure the lateral visual field by coupling the eyelids, but without distortion of the canthal angle and eyelid margin. The procedure is often coupled with a lateral canthoplasty or canthopexy to address horizontal laxity of the lower eyelid. Collecting standardized outcome measures will help establish the ideal treatment paradigm of paralytic eyelid malposition.
Key points
- •
Eyelid coupling using the modified tarsoconjunctival flap is an effective treatment for paralytic ectropion.
- •
Eyelid position and quality of life can be improved in patients with flaccid facial paralysis using these eyelid coupling procedures.
- •
The modified tarsoconjunctival flap can obscure the lateral visual field by coupling the eyelids, but without distortion of the canthal angle and eyelid margin.
- •
The procedure is often coupled with a lateral canthoplasty or canthopexy to address horizontal laxity of the lower eyelid.
- •
Collecting standardized outcome measures will help establish the ideal treatment paradigm of paralytic eyelid malposition.
Introduction
The primary function of the eyelids is to maintain ocular health and protection. The natural blink mechanism provides the eye with a protective tear film, prevents corneal desiccation and injury, and facilitates the flow of tears. Eyelid function relies on a complex array of muscles that retract and elevate in coordinated fashion. Patients with facial paralysis lose that coordinated function and can present with profound ocular sequelae. Most notable is the loss of sphincter function of the orbicularis oculi muscle.
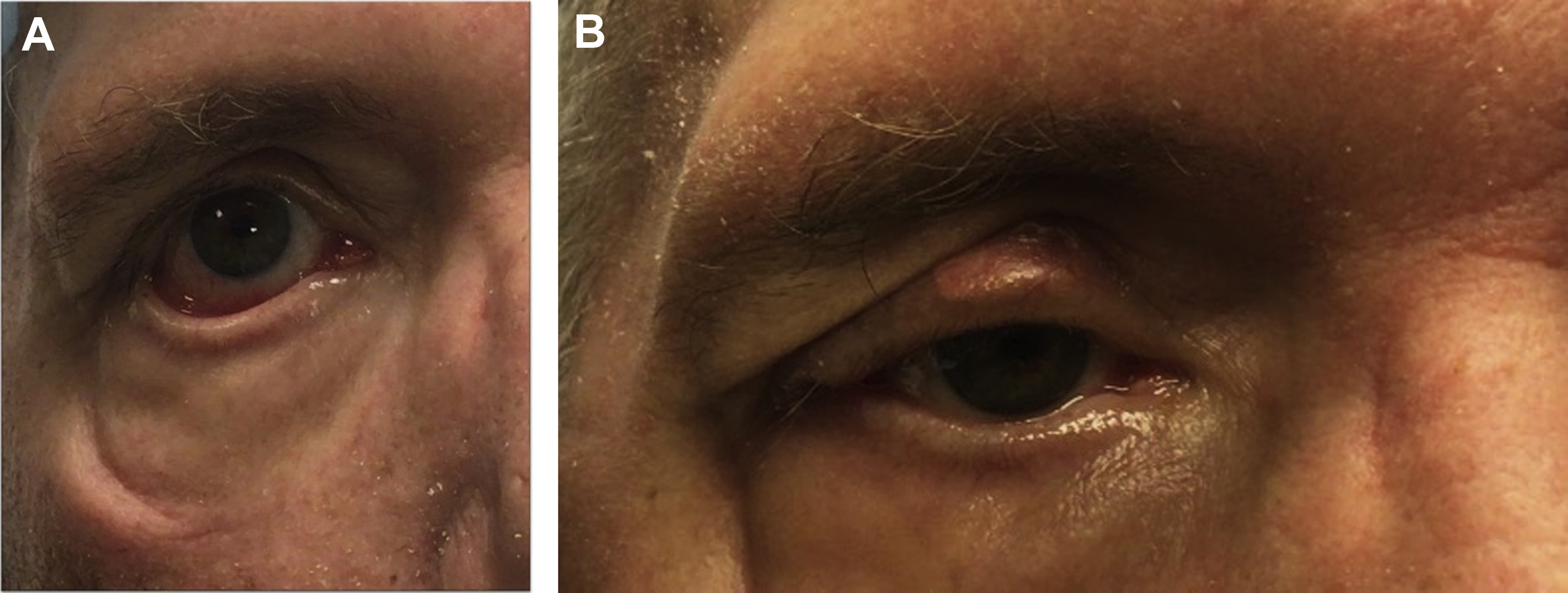
In the paralyzed face, loss of orbicularis oculi function results in unopposed action of the upper-eyelid retractors (levator palpebrae superioris and Mullers muscle) and lower-eyelid retractors (inferior tarsal muscle). This subsequently leads to an increase in palpebral fissure height and lagophthalmos, which put the eye at risk for complications from exposure. Other factors, such as age, scarring, or radiation therapy, can affect eyelid function and exacerbate the functional impairment. Impaired blink from dynamic dysfunction of the eyelids results in poor tear film distribution and clearance through the lacrimal pump. This may manifest in epiphora, presence of a tear lake, and dryness from ineffective ocular lubrication. Corneal protection by limiting lagophthalmos is important to prevent exposure keratopathy. Lower-eyelid malposition is a major contributor to ocular sequalae of facial paralysis and is characterized by paralytic ectropion and retraction. The ectropion demonstrates eyelid eversion, whereas retraction is seen as downward gravitational pull on the eyelid ( Fig. 1 A).
The goals of treating the paralyzed eyelid complex are to protect the cornea and restore facial symmetry. Initial management frequently includes a moisture chamber and ocular lubrication to protect the cornea. Further intervention typically involves a combined approach to the upper and lower eyelids. For patients with suspected transient facial paresis, options include eyelid taping, temporary tarsorrhaphy, and induction of protective upper-eyelid ptosis with botulinum toxin. For chronic facial paralysis, upper-eyelid loading aids the retracted eyelid and helps prevent lagophthalmos. To address lower-eyelid malposition, a spectrum of techniques has been described that (1) shorten and/or tighten the lower eyelid, (2) suspend the lower eyelid, (3) support the middle lamella, (4) release retractors of the lower eyelid, or (5) connect the lower and upper eyelids. ,
For chronic, flaccid facial paralysis, early postoperative success is often marred by inadequate eyelid position over time. The need for imporved long-term outcomes explains the continued pursuit of novel and modified eyelid procedures to treat paralytic ectropion. The authors of this article have favored an eyelid-coupling procedure using the modified tarsoconjunctival flap to correct paralytic ectropion. , The procedure is often used in conjunction with a lateral strip canthoplasty to address horizontal laxity. The modified tarsoconjunctival flap couples and balances the effect of the previously unopposed upper- and lower-eyelid retractors, thereby improving eyelid malposition and lagophthalmos. The flap also provides a vertical vector of support to the lower eyelid that is not provided by the lateral strip canthoplasty alone. Finally, the coupling provides dynamic benefit by allowing the upper-eyelid retractors to raise the lower eyelid (and vice versa), improving tear film distribution (eg, the squeegee effect). The modified tarsoconjunctival flap has advantages over traditional eyelid coupling surgery (eg, tarsorrhaphy), as it does create less distortion than the canthal angle and eyelid and is easily reversible (see Fig. 1 B). Here, the authors describe their surgical technique and discuss patient outcomes.
Surgical technique
Lateral eyelid coupling is accomplished by insetting an upper-eyelid tarsoconjunctival flap into the lower eyelid. This procedure is frequently combined with either a lateral tarsal strip canthoplasty or a canthopexy with lateral retinacular suspension to address horizontal laxity. The tarsal strip canthoplasty differs from a canthopexy by including a through-and-through canthotomy/cantholysis. The canthopexy is achieved by using a lateral canthal skin incision to approach the inferior limb of the lateral canthal tendon, which is suspended upward and laterally with a suture to the medial aspect of the lateral orbital wall.
There are 4 main steps to this procedure:
- (1)
Create a tarsal strip or expose the lateral retinacular suspension
- (2)
Elevate a superiorly based tarsoconjunctival flap from the upper eyelid
- (3)
Inset tarsoconjunctival flap into the lower eyelid
- (4)
Suspend the lateral canthal tendon to the lateral orbit (canthoplasty or canthopexy)
In step 1, the lateral canthotomy and inferior cantholysis are performed. Once the lower eyelid is free from its attachment to Whitnall tubercle, the lateral canthal tendon is then prepared by denuding the lateral skin and conjunctiva. A full-thickness excision of the lateral canthal tendon is performed to the degree needed to correct lower-eyelid laxity. The canthoplasty or canthopexy suture is parachuted in horizontal mattress fashion with either a 5-0 Polydiaxanone or 5-0 Poly(ethylene terephthalate) suture through the lateral canthal tendon and lateral orbital rim periosteum (superior and posterior to Whitnall tubercle). The suture is placed at this time, as it is more difficult to place once the tarsoconjunctival flap has been inset. This suture suspension of the lateral canthus is not tied until step 4.
In step 2, the upper eyelid is inverted over a DesMarres retractor using a 4-0 silk traction suture placed through the gray line. Hydrodissection with local anesthetic of the upper-eyelid tarsoconjunctival flap assists with flap elevation. The superiorly based flap is planned at the lateral aspect of the upper eyelid. The flap is designed to be 3 to 8 mm wide (adjustable to severity of eyelid laxity and snap test result) and 4 mm tall and includes the superior 1 to 2 mm of the tarsal plate ( Fig. 2 ).

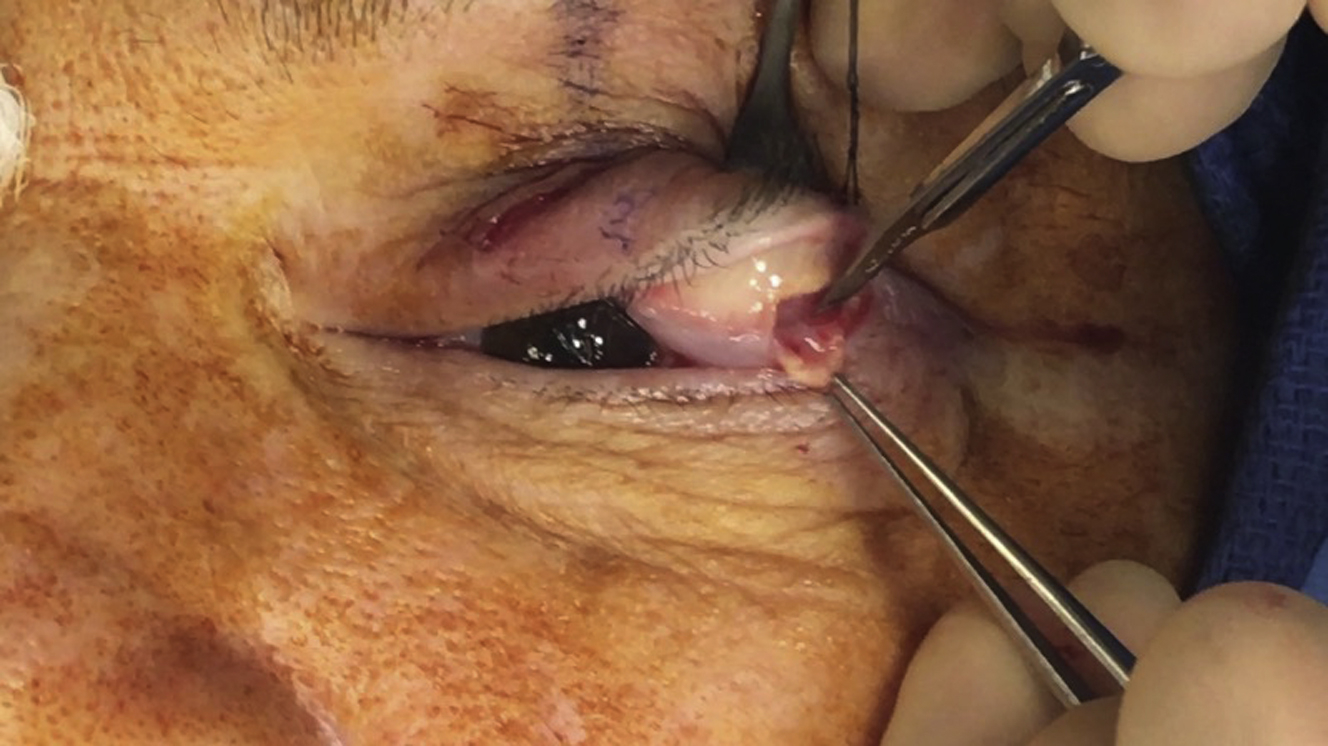
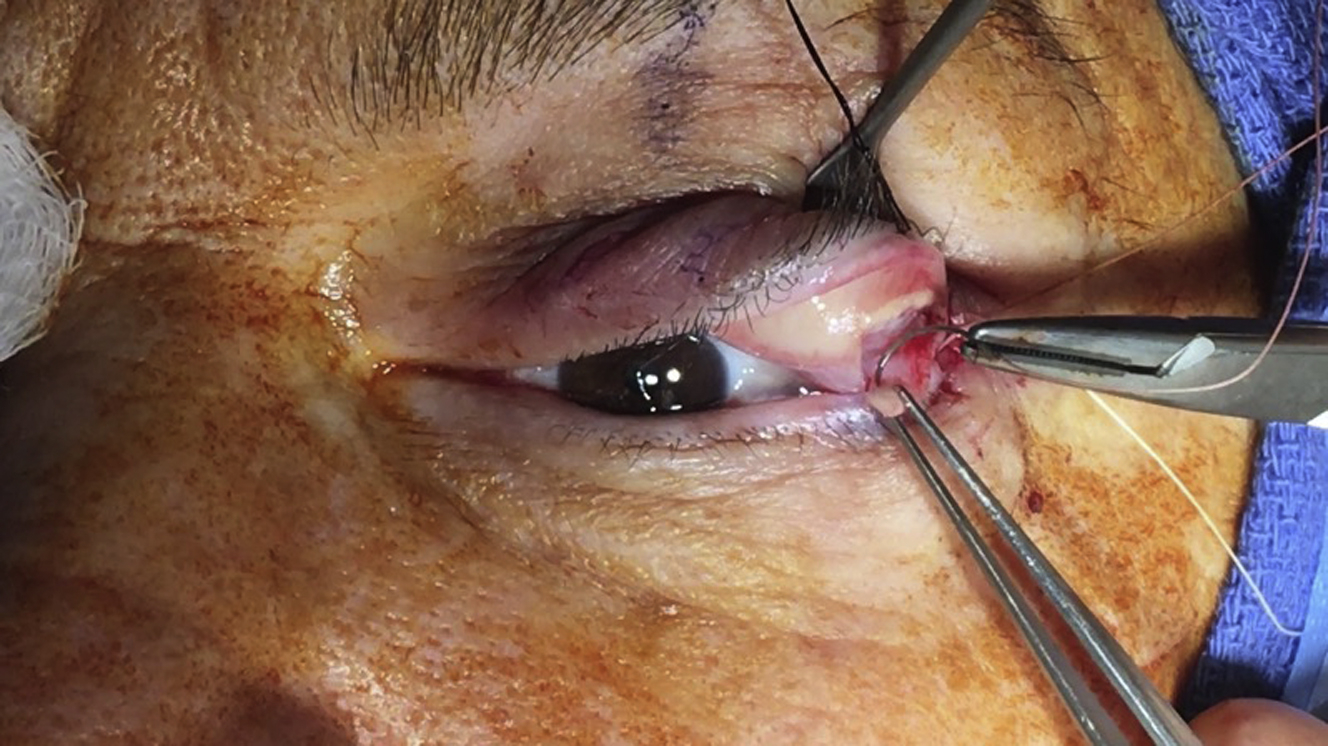
In step 3, an incision is made at the gray line at the lateral aspect of the lower eyelid, and a small sliver of lid margin is denuded to create a pocket to inset the tarsoconjunctival flap. The flap is then elevated and brought down in the usual fashion for a modified Hughes tarsoconjunctival flap ( Fig. 3 ) and sutured into the pocket with 4-0 polygalactin suture in interrupted fashion ( Fig. 4 ). To prevent ocular injury or irritation, it is key to place the knots facing away from sclera.
In step 4, the canthoplasty or canthopexy suture placed in step 1 is then tied down. The lateral canthal angle can be re-created with a 6-0 fast-absorbing gut suture, which is secured under the 6-0 silk sutures used for the skin layer of the canthotomy/canthopexy closure. Before the skin closure, a deep layer with interrupted 5-0 Poliglecaprone sutures is used to approximate the wound edges.
Discussion
There is no absolutely effective treatment for the eyelid manifestations of facial paralysis for all patients. The surgical techniques used are varied based on the severity of the paralysis, senile changes to the eyelids, and anatomic variations (eg, negative vector midface position). Comparing the reported techniques has been difficult because of dogma and a lack of uniform outcome measures reported in the literature.
Growing experience with the modified tarsoconjunctival flap is evident in the literature. Tao and colleagues published the largest series (n = 110) of patients undergoing tarsoconjunctival flaps for paralytic ectropion. The procedure was combined with a lateral canthoplasty (n = 45) when horizontal laxity was identified. In their cohort, lagophthalmos, exposure keratopathy, and eyelid retraction improved in all cases. The investigators describe an additional dynamic benefit, especially in patients with a strong Bell reflex, as the lower eyelid elevated during upward movement of the eye. It is postulated that this finding may be secondary to the flap’s attachments to the fornix. Although these results favor the use of this technique, the lack of reported facial paralysis severity and quantifiable patient-reported outcome measures (PROM) prevent generalized application to facial paralysis patients.
The Facial Clinimetric Evaluation (FaCE) instrument is a patient-reported quality-of-life metric that scores facial movement, facial comfort, oral function, eye comfort, lacrimal control, and social function. Dedhia and colleagues reported their modified tarsoconjunctival flap outcomes in patients with flaccid facial paralysis using the FaCE instrument and ectropion grading scale (EGS). The outcomes were stratified by those that received periorbital or midface radiation therapy. Patients who had received radiation therapy demonstrated improvement in eye comfort and lacrimal control subdomain scores of the FaCE instrument, whereas no difference was seen in patients who had not undergone radiation therapy; all patients had improved eyelid position as graded by the EGS. Outcomes from future studies on paralytic ectropion that report these standardized metrics (ie, FaCE scale and EGS) can be used to compare efficacy of treatment and help elucidate which procedures are optimal for a given patient.
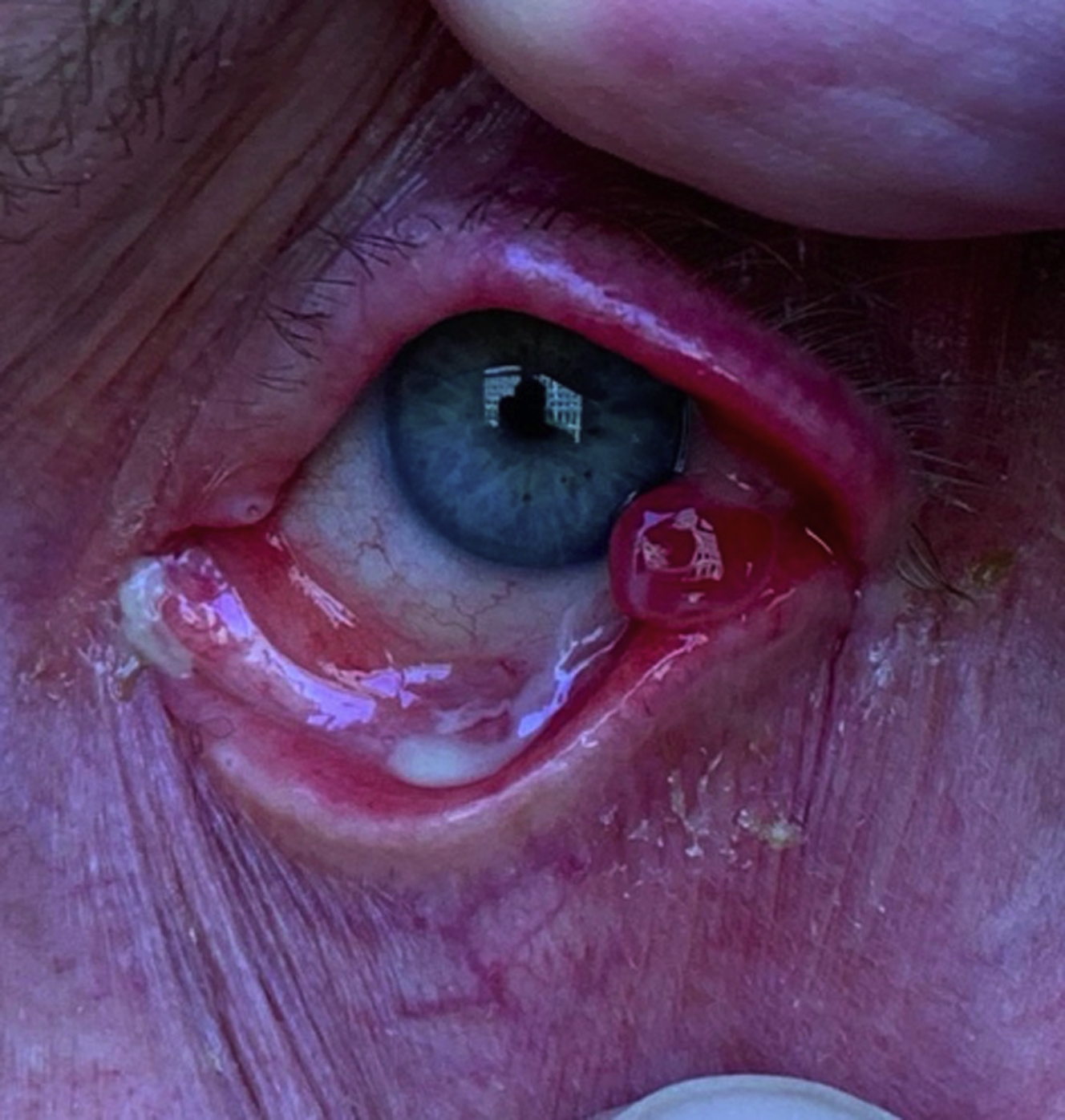
Complications with the tarsoconjunctival flap are rare. The authors’ experience is consistent with that which has been previously reported by Tao and colleagues, who reported a flap dehiscence rate of 2.6%, which was easily treated with repeat suturing; pyogenic granuloma rate of 4.5%, which required excision; and loss of peripheral vision rate of 6.4%, which was treated with partial flap division under local anesthesia. In the authors’ experience, around 10% of cases develop a temporary granulation tissue, consistent with pyogenic granuloma ( Fig. 5 ). Patients will complain of dried crusting of the lateral canthal region and are amenable to antibiotic/steroid ointments or drops. Most likely, these are normal healing responses to the polygalactin sutures used for the closure.
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Dual Nerve Transfer for Facial Reanimation
Dual Nerve Transfer for Facial Reanimation
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
 Facial Reanimation and Reconstruction of the Radical Parotidectomy
Facial Reanimation and Reconstruction of the Radical Parotidectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


