Epiblepharon
Adam R. Sweeney
Christopher B. Chambers
DEFINITION
Epiblepharon is a congenital eyelid anomaly in which inward rotation of the normal lash line toward the globe results in eyelash approximation to the cornea and/or conjunctiva.
ANATOMY
A horizontal eyelid fold composed of skin and orbicularis is evident inferior to the eyelid margin. This is caused by the absence of the adhesion between the thin smooth muscle contributing to lower eyelid retraction and the soft tissue immediately deep to the lower eyelid skin.1,2
Often, the fold is more pronounced or isolated to the medial eyelid.
The Asian lower eyelid has a higher attachment of the septum on the tarsus or inferior retractor. Additionally, there often is an absence or paucity of retractor septa attached to the overlying skin, similar to the Asian upper eyelid.1
The tarsus is not rolled in, nor is there rotation of the eyelid muscle, separating this condition from entropion.3
PATHOGENESIS
Epiblepharon is one of the most common eyelid abnormalities among Asian children, with majority demonstrating spontaneous resolution throughout childhood.4
Epiblepharon much more commonly involves the lower eyelid than it does both upper and lower eyelids with a small minority of cases involving solely the upper eyelid.2
There is no gender predilection.2
Epiblepharon is less commonly seen in adults.
Asian children with higher BMI are more likely to have epiblepharon.6
Acquired epiblepharon is rare and often secondary to thyroid eye disease.7
NATURAL HISTORY
The majority of patients will have spontaneous resolution with growth of the midface stretching and flattening the redundant fold.
Patients with untreated epiblepharon may have a continuum of sequelae with some asymptomatic until development of thicker eyelashes, whereas others may develop conjunctival epithelial defects, corneal defects, recurrent corneal infections, and even corneal scarring.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients may be asymptomatic or have inciting surface irritation evident by rubbing of eyes, photophobia, persistent tearing, or discharge.
Eyelashes may be vertically oriented and may touch the cornea. This often is exacerbated in down gaze.
Fluorescein staining may reveal epithelial defects.
Epiblepharon may be associated with astigmatism.
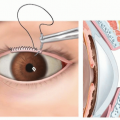
Diagnosis is by physical exam with the eyelashes directed vertically in the setting of normal eyelid position (FIG 1). Additionally, an eyelid fold may be found to be mechanically corrected with downward pressure applied on the skin away from the eyelid involved.
IMAGING
Preoperative quality external photos documenting resolution of the epiblepharon with eyelid fold excursion are recommended prior to undergoing surgery.
DIFFERENTIAL DIAGNOSIS
Entropion with or without epiblepharon
Trichiasis, or misdirected growth of eyelashes toward the eye
Epicanthus tarsalis
Dermatochalasis with lash ptosis
Ptosis
Discharge in nonverbal children may be a sign of backflow from the tear drainage pathway, caused by nasolacrimal duct obstruction.
 FIG 1 • Lower lid epiblepharon. Eyelashes are seen directed vertically with inferior eyelid fold. |
NONOPERATIVE MANAGEMENT
Monitoring is appropriate in asymptomatic cases without corneal eyelash apposition.
Lubrication with scheduled artificial tears may suffice in asymptomatic cases with mild epiblepharon or conjunctival eyelash apposition.
SURGICAL MANAGEMENT
Preoperative Planning
General anesthesia is recommended for pediatric cases.
Surgical intervention is warranted in children whose lid abnormality causes keratopathy or conjunctivopathy, considerable irritation, or in cases where lubrication is not tolerated.
Goals of surgical management are to achieve eyelid retractor tightening, removal of a strip of orbicularis and skin, and creation of a scar in a region between the preseptal and pretarsal orbicularis.
In patients for whom a surgical eyelid crease is not desired, the standard technique for epiblepharon is used. If a surgical eyelid crease is desired, the modified Hotz technique is used.
A noninvasive everting suture technique may be offered. This modality may be appropriate for mild cases of epiblepharon, parents wishing to avoid creation of an eyelid crease/scar, or avoidance of general anesthesia.
Positioning
The patient is positioned supine on a surgical table with an adjustable headrest lowered to give the surgeon the best access. The patient should be prepped and draped, leaving the full face exposed.
Approach
An external approach to the lower lid tarsus and eyelid retractors is classically used. Alternatively, a noninvasive suture technique may also be used.
TECHNIQUES
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


