Chapter 24 Endoscopic plication techniques for the treatment of abdominal contour
Basic Science
The correction of the diastasis can be accomplished via a small video-assisted suprapubic incision, without skin resection, or by a mini-abdominoplasty in a technique described since 1971 by Callia, with a small infraumbilical skin resection. Other authors have already described, with variations, an infraumbilical plication only and no detachment of the umbilicus.1–7 There are also descriptions of a small incision in the umbilicus to facilitate the supraumbilical detachment2 and another approach that detached the umbilicus from the m. rectus.8,9 Since the introduction of video-endoscopy, indications for the correction of diastasis without skin resection can be extended to include, primarily, congenital diastasis and diastasis in men.10
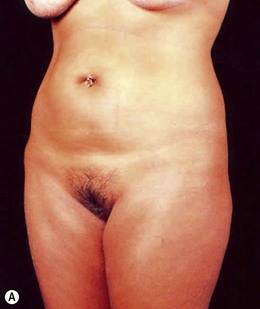
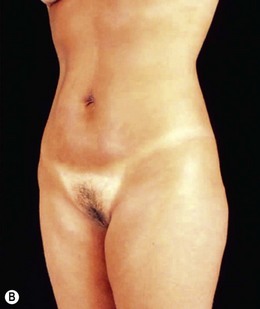
Indications for video-assisted mini-abdominoplasty are limited. This option must be precisely discussed with the patient because, on the one hand, there is the advantage of less scarring, but on the other hand, resection of skin is limited and there may be mild residual laxity both above and below the umbilicus. Another factor that should be considered in female patients is the possibility of pregnancy after surgery. In nulliparous patients who have abdominal flaccidity following weight loss (Figs 24.1 and 24.2), or in patients who have post-pregnancy abdominal flaccidity but are planning another pregnancy, this technique would be well indicated, because it doesn’t present the same limitations as classical abdominoplasty for postoperative pregnancy.
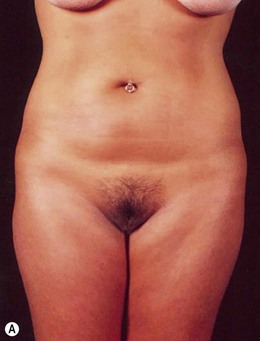
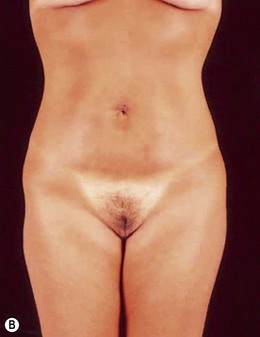
FIG 24.2 Appears  ONLINE ONLY
ONLINE ONLY
Patient Selection
The selection of patients is subject to strict criteria:
• Patients with mild supra- and/or infraumbilical skin laxity, with diastasis of the rectus abdominis.
• High navel position, more than 14 cm above the pubis.
• Firm or minimally flaccid supraumbilical skin that will not allow the descent of the supraumbilical region to the suprapubic region.
• The possibility of post-abdominoplasty pregnancy, provided that the flaccidity is not excessive. These patients fall into Types III and IV of the Bozola and Psillakis classifications,1 and Type I in the Nahas classification system.4
• Diastasis of the rectus abdominis muscle, which can either be acquired (post-pregnancy or following weight loss), or congenital, which can occur in both women and men (Figs 24.1–24.7).








FIG 24.4 Appears  ONLINE ONLY
ONLINE ONLY
• Abdominal hernias (especially umbilical hernia) associated with lipodystrophy and skin flaccidity (Figs 24.8 and 24.9).
• Lipodystrophy and moderate skin flaccidity, where liposuction would offer limited results (Figs 24.10 and 24.11). Younger patients who have undergone massive weight loss resulting in abdominal flaccidity fall into this category, and also those with post-pregnancy flaccidity but who may become pregnant in the future (Figs 24.12 and 24.13).
< div class='tao-gold-member'>







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


