Chapter 31 Liposuction of the abdomen and trunk
• Liposuction is one of the most common esthetic procedures performed and the incidence of complications is low.
• Liposuction is more of an art than a surgical procedure.
• Liposuction entails a practical application of scientific knowledge with precision and craftsmanship and is a skill attained with clinical experience.
• In this chapter the technique, the pearls and the pitfalls of liposuction are described in detail. A series of patients who underwent liposuction of abdomen and trunk are presented.
• The long-term results of liposuction depend on the preoperative condition of the patient’s skin, the patient’s overall health and expectations, and the ability of the patient to maintain a healthy weight and lifestyle postoperatively.
Introduction
Concepts of beauty have been continuously evolving throughout the history of mankind. The voluptuous figures that were idealized by artists in the past have been substituted by slimmer forms. In many countries, liposuction is the most frequently performed esthetic procedure.1,2 Liposuction has evolved tremendously over the past three decades. Since its introduction, it has progressed into one of the most popular procedures in plastic surgery.3,4 The “Illouz Method” featured a technique of suction-assisted lipolysis after infusing fluid into tissues using blunt cannulas and high-vacuum suction and demonstrated both reproducible good results and low morbidity. Liposuction is more of an art than a surgical procedure. It entails a practical application of scientific knowledge with precision and craftsmanship and is a skill attained with clinical experience. The development of liposuction provided plastic surgeons with a safe and effective way to sculpt the human figure.5 It brings as much contentment and joy to the person undergoing it, as to the surgeon practicing the intimidating task of delivering that eventual result. The goal of liposuction is the reduction of localized fatty tissue to produce well-proportioned body contours. Although liposuction has been considered a safe surgical procedure for the last 30 years, to maximally avoid complications, one should be mindful of all the factors that could predispose to them.6
Preoperative Preparation
• Significant medical conditions that may be aggravated by surgery or anesthesia, and use of all medications, vitamins and herbs must be documented.
• Local conditions of skin or subcutaneous tissue that make liposuction hazardous.
• Psychological contraindications such as mood disorders, thought disorders, severe anxiety, or unrealistic expectations.
Appropriate indications should be recorded in the clinical record which may include:
• The removal of localized or regional deposits of adipose tissue for the purpose of body contouring.
• The treatment of specific conditions of adipose and subcutaneous tissues but not the management of obesity.
Surgical Technique
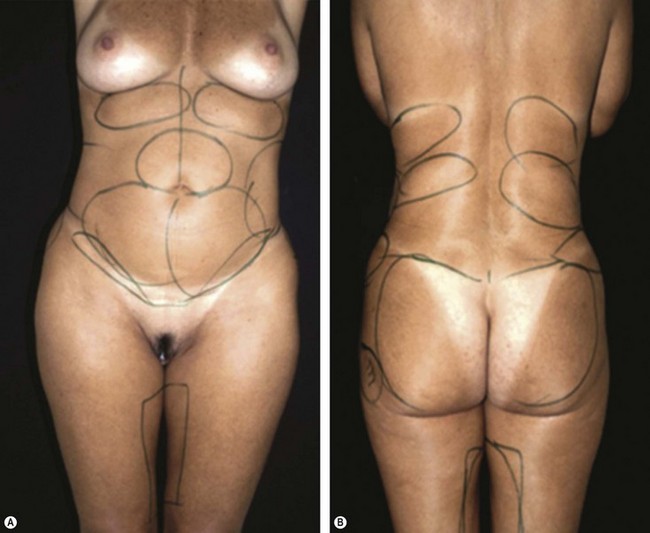
1. Markings of the areas to be liposuctioned and fat grafted are made while the patient is in the standing position (Fig. 31.1A, B).
2. Preoperative sedation in the surgical suite is administered. Anesthesia consists of an epidural block and intravenous sedation. The patient is placed in supine position.
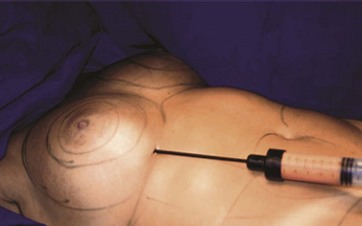
3. After the injection of normal saline wetting solution containing 1 : 500 000 of epinephrine (adrenaline) by a small-bore cannula and waiting 15 minutes, a 60 ml syringe attached to a 4 mm blunt cannula is inserted through two small incisions in the area to be liposuctioned.
4. Fat is aspirated using the syringe method in the dorsum and the flanks (Fig. 31.2).
5. If autologous fat transfer is being considered, the aspirated fatty tissue is treated in the following manner: With the syringe held vertically with the open end down, the fat and fluid are separated. Isotonic saline is added to the syringe, the fat and saline are separated and the exudate discarded. The procedure is repeated until the fat becomes yellow in color, free of blood and triglyceride oil. Our experience with autologous fat transplantation in treating various tissue defects has been published previously.7–9
6. When gluteal augmentation is scheduled, a deep plane to the gluteal muscles is created by the 4 mm cannula. Then other planes are created by the same cannula in different trajectories, always from the deeper aspect to the gluteal surface. The fat is inserted into these tunnels beginning at the deep layer and working up into the intermediate fat compartments. The fat is injected as the cannula is withdrawn. Care should be taken to avoid injection of more fat in the superficial fat compartment. Separate incisions, if necessary can be used to treat the whole gluteal region (Fig. 31.3).
7. When needed, fat grafting to the female breast (Fig. 31.4) and liposuction to the abdomen is then performed (Fig. 31.5). When indicated, lipoabdominoplasty is performed. The combination of circumferential liposuction, fat grafting of the buttocks and lower limbs, and modified transverse abdominoplasty has been described as composite body contouring in the literature.10
8. The patient remains hospitalized for 24 hours. Antibiotics, analgesics and anti-inflammatory medications are prescribed during the following 7 postoperative days.



A video demonstrating the technique is presented.
Nine illustrative cases are presented.
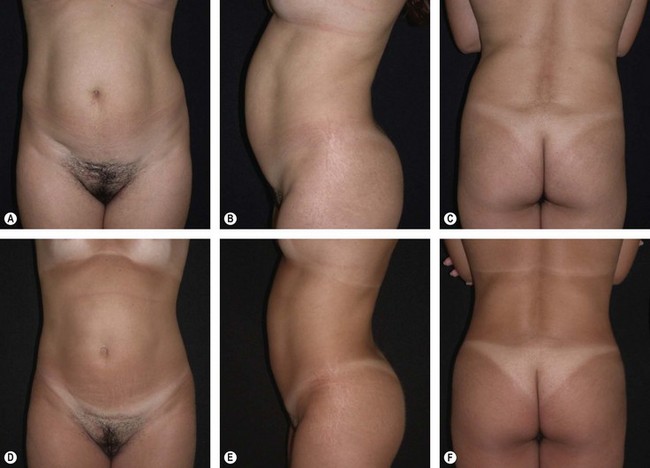
Case 1
This 24-year-old lady presented complaining of “extra fat” which made her “unattractive” (Fig. 31.6A–C). Liposuction of the back, flanks, and abdomen and autologous gluteal lipograft was performed. Photos were taken 3 years after the procedure (Fig. 31.6D–F). Breast augmentation by silicone implant was also performed.
< div class='tao-gold-member'>
Related posts:
 Brachioplasty with liposuction resection
Brachioplasty with liposuction resection
 Tumescent local anesthesia for liposuction
Tumescent local anesthesia for liposuction
 Lipoabdominoplasty with previous flap resection
Lipoabdominoplasty with previous flap resection
 Autologous gluteal augmentation with mid-pedicle superior pole perforator flaps
Autologous gluteal augmentation with mid-pedicle superior pole perforator flaps
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


