Chapter 22 Lipoabdominoplasty with previous flap resection
• Lipoabdominoplasty with previous flap resection is a complete method for the correction of esthetic abdominal deformities by removing excess skin and subcutaneous fat whilst also repairing the rectus diastasis and tissue laxity.
• Abdominal surgery has been extensively revised and published since Dermars and Marx in 1890 and Kelly1 in 1899.
• It is important to note the following:
Introduction
Surgeons such as Callia,2 Pitanguy,3 Pontes,4 Baroudi,5 Avelar,6 Matarasso,7 Lockwood,8 Guerrero Santos,9 and many others around the world have contributed to the development of surgery in the abdominal area.
Concerning vascularization studies, contributions from El Mrakbey,10 Boyd and Taylor11 and others have highlighted the associated morbidity related to the extension of the undermining in these procedures.
The classifications of the pathology, according to Pitanguy12 and Bozola,13 allowed more precise and correct surgical indication by choosing the technical options and the extension of each procedure.
Baroudi’s5 stitch technique greatly diminished the occurrence of seroma formation by plicating the abdominal flap to the aponeurosis. Seroma formation, together with infection and skin necrosis, are the major complications of this procedure in the postoperative period.
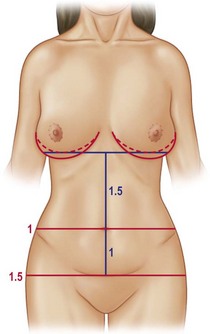
Bozola13 described the umbilical position, which can be measured in a geometric proportion of 1 for the infraumbilical portion and 1.5 for the supraumbilical area, giving a harmonic relationship to the abdomen (Fig. 22.1). The umbilical position will be the parameter for our assessment concerning the removal of the infraumbilical flap, so we must be extremely careful with those patients having a high umbilical scar position.
However, the greatest advancement in the evolution of abdominoplasty was the use of liposuction. The liposuction studies by Illouz,14 Avelar,6 Saldanha,15 Hunstad16 and Klein17 highlighted the safety of this procedure in regular association with traditional abdominoplasty. Liposuction decreases fat thickness and reduces the undermining required. This results in both harmonious and satisfactory outcomes for the patients and their respective surgeons.
In our clinical practice we are in favor of the previous resection of the abdominal flap as proposed by Pontes4 since 1964. The ease of the resection, the absolute control of bleeding, scar symmetry, and improved speed and efficiency of the procedure are our critical points to advocate the abdominoplasty with previous flap resection as our routine technique. In addition, improved flap handling is another distinct advantage and further emphasizes our preference for this procedure.
Preoperative Preparation
Patient Selection
Type I: Abdominal lipodystrophy without skin flaccidity, absence of diastasis or hernia, umbilical scar in normal anatomical position.
Type II: Infraumbilical abdominal lipodystrophy with discrete cutaneous flaccidity, presence or absence of diastasis, umbilical scar in normal anatomical position.
Type III: Generalized abdominal lipodystrophy with moderate cutaneous flaccidity, and presence or absence of diastasis.
Type IIIA: Umbilical scar in normal anatomical position.
Type IIIB: Umbilical scar in excessively high anatomical position.
Type IV: Abdominal lipodystrophy with marked cutaneous flaccidity, the presence of muscular diastasis or eventrations with or without associated umbilical scar in a normal anatomical position.
Type V: Marked abdominal cutaneous flaccidity with or without lipodystrophy; presence of scar at the midline of the abdomen. The umbilical position is in a normal or altered anatomical position.
Type VI: Marked generalized abdominal lipodystrophy and flaccidity. These patients are generally not considered good candidates for an esthetic surgical procedure. Patients in this group should undergo a strict clinical treatment to lose weight, frequently needing the attention of a multidisciplinary team (e.g., endocrinologist, physiotherapist, nutritionist, physiologist, etc.).
So, with precise analysis we can choose the exact surgery type for each case.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


