Chapter 36 Short vertical scar medial thigh lift
Introduction
Lax tissues in the upper thigh can be a concern to many people, particularly where there has been significant weight loss.1 Rubbing inner thighs can cause sores and hygiene problems. The esthetic consequences of redundant skin can be a major psychological disability and destroy interpersonal relationships.
In my experience, there is an inevitable gravitational drag on tissue that is undergoing repair and if the holding suture fails and an excessive amount of “thigh lift” has been performed, then the labia majora is pulled down, causing an open introitus and a severe problem with underwear and hygiene.2 Whilst there may be a good initial result, it becomes certain that an undesirable scar occurs below the bikini line. The presence of labial skin in the inner thigh is a major disaster.
Applied Anatomy
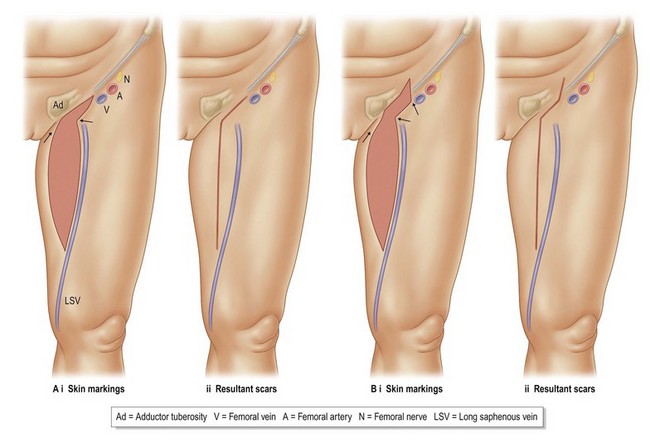
The mons pubis is held in an elevated position by fibrous suspensory attachments, but these generally loosen off with ageing and weight loss. The descent of the mons and tissues immediately above the inguinal ligament starts the cascade that results in soft tissue redundancy at a level usually at the apex of the femoral triangle. Simply lifting the mons, as occurs in some forms of abdominoplasty, can improve the appearance of the inner thigh. For a long-lasting effect though, a vertical narrowing of the base of the cone is required and this can be achieved in a number of ways (Fig. 36.1). In the tissues over the femoral triangle there are a significant number of important structures that should be maintained if possible.
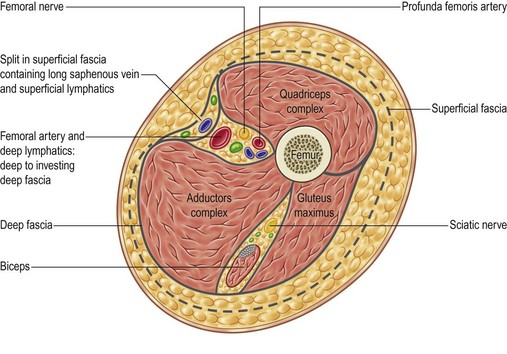
The long saphenous vein passes upwards from a point one hand’s breadth behind the medial border of the patella, to a point two fingers breadth below and two fingers breadth lateral to the pubic tubercle. The vein then turns 90° through the cribriform fascia, so joining the femoral vein at the saphenofemoral junction. The vein passes beneath the Scarpa’s fascia in its vertical ascent and is superficial to deep fascia (Fig. 36.2).
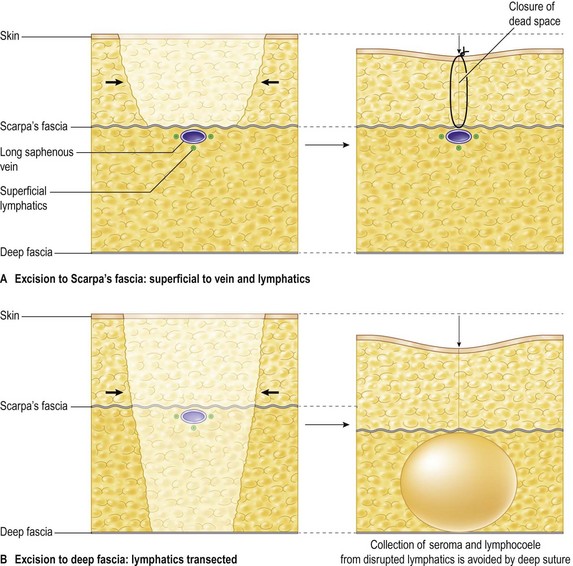
Superficial lymphatics in the thigh travel alongside the saphenous vein as trunks, before separating from the vein to enter the femoral ring and passing through a complex of lymph nodes, the most well known being Cloquet’s gland. Superficial lower leg lymph vessels follow the long saphenous vein medially and are larger and more numerous than the lower leg lateral lymphatics that pass deeply into the popliteal fossa. The medial thigh lymphatics ascend to the lower group of inguinal lymph nodes. Superficial lymphatics around the posterior thigh and buttocks pass medially and anteriorly to the front of the thigh and terminate in the upper group of inguinal nodes. By restricting the depth of resection, the undermining of tissues and the extent of the wound, there is less likelihood of lymphatic damage and subsequent collection of lymph with subsequent morbidity. The excisional plane, therefore, must be superficial to the long saphenous vein. Contrary to common procedure, it is important to preserve bulk to the thigh whilst performing the lift. For example, in the Brazilian abdominoplasty3 there is preservation of all tissues above Scarpa’s fascia and there is no incidence of seroma or lymphocele. Similarly, in the groin, if lymphatics are preserved by using lipomobilization techniques, there is no dead space available to create a problem with fluid collections in the thigh (Fig. 36.3).
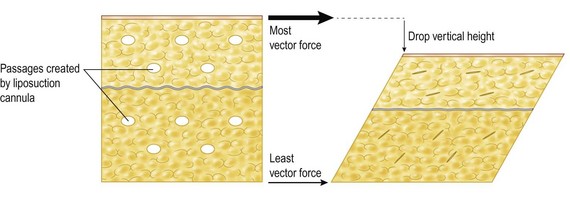
If there is a minimal undermining of tissue there is no possibility of wound edge necrosis as was commonly seen after groin dissection without a 2 cm skin edge resection for malignancy.4 As the skin is approximated, the deeper tissues tighten under compression (Fig. 36.4). This will loosen eventually but still leave a better result than after a major debulking of the medial thigh tissues.
Surgical Technique
Immediately prior to surgery the patient is marked in a standing position and the problem area is addressed (Figs 36.5 and 36.6). Scars are limited in vertical length within the medial aspect of the thigh then curve anteriorly to follow the groin crease for a few centimeters, before ascending vertically again into the mons pubis in cases where there is significant mons ptosis and redundancy, the skin markings are as in Fig. 36.1. The surface marking of the long saphenous vein is noted and the proposed skin excision is marked accordingly. In the short vertical scar inner thigh lift the skin paddle excision will extend to a thigh level just distal to the apex of the femoral triangle. Variances to the scar are created by several choices of design in the skin paddle excisions. In general, a horizontal groin crease scar will drop and widen unless there is a vertical element above it, or if the horizontal scar can be restricted. Not all vertical scar thigh lifts require an extension into the mons pubis.
< div class='tao-gold-member'>

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


