Chapter 17 Upper body lift with lateral excision
• Upper body lift. This combination of single procedures is described and compared to single stage techniques.
• The main technical aspects are highlighted and described in the clinical context.
• Prevention, reduction and management of complications are demonstrated for this specific procedure.
• Different intraoperative steps are explained to enable procedure enhancement.
• The combination of liposuction and upper body contouring procedures has to be performed cautiously and restricted. Therefore, limitations are emphasized.
Introduction
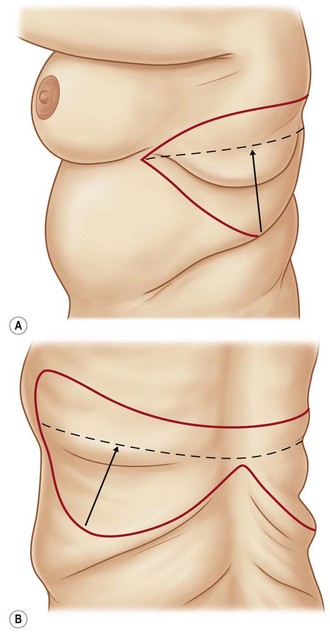
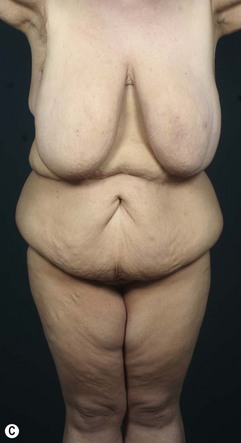
In the past, reconstructive operations such as breast reshaping, arm- and back-lifts were performed as single-stage procedures, especially for patients after massive weight loss. As part of a progression in this specific subfield of plastic surgery, modern treatment concepts have been established, such as the upper body lift, with or without a circumferential upper thoracic lift.1–7 Besides the reconstruction of the breast with implants or alternatively with autologous tissues from the upper abdomen and/or lateral thorax, these regions can be sufficiently tightened in a single procedure, positioning the scar as a continuation of the submammary fold, ascending to the axillary crease. Patients with mild to moderate skin and tissue excess in the dorsal thoracic region can benefit from a sufficient skin tightening in this area by this approach. The upper arm reconstruction can easily be continued, without any interaction with the axillary reconstruction. In individual cases with severe skin excess at the dorsal thorax, a direct approach in terms of a bra-line lift can be performed4 (Fig. 17.1).


Preoperative Preparation
For general information please refer to Chapter 38.
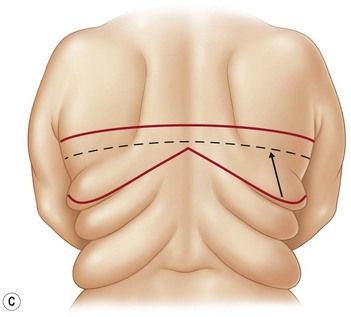
The decision for an upper body lift is made on the extent of skin and soft tissue excess at the lateral and dorsal thoracic wall. The classification of the lateral folds after massive weight loss is designated by Strauch et al into an upper breast roll, followed by a lower scapular roll or a deeper lower chest/thoracic roll. An analogous classification is made for the iliac area as hip rolls. The folds can be seen individually, often with a fluent passage.8 The two upper folds often can be treated by various surgical options and are only peripherally influenced by the lower body lift alone, whereas the two lower folds can only effectively be treated by a lower body lift or a belt lipectomy (Fig. 17.2).
Markings
Marking of the breast procedure is performed so that it is personalized to the patient. Regarding the new nipple–areola complex position, we emphasize the measurement of it proportional to the submammary fold and the upper breast border. Since women with low submammary folds have an appropriately low upper breast border, a high nipple–areola complex may lead to an early postoperative bottoming out. We prefer the central pedicle with dermal suspension as presented by Rubin and the double-ellipse technique for the arm reconstruction as published by Aly.2,9
This maneuver allows a transposition and rotation of the lateral and dorsal soft-tissue cranial and anterior, with a resulting scar that is located at the medial or posterior axillary line. The lateral tension from the back may cause a lateralization of the breast which must be considered during the markings for the breast. The position of the nipple–areola complex should always be double-checked after finishing the upper lateral-thoracic-lift.4–6
Surgical Technique
Upper Lateral Thoracic Lift
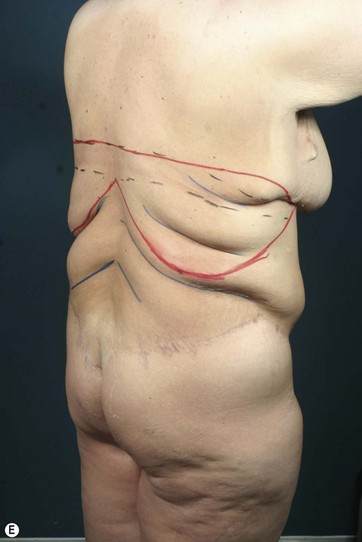
The conventional surgical treatment of the upper two back and lateral rolls by direct excision at the aspect of the dorsal thorax often leads to wide, unsightly and permanent visible scars. Respecting the different interfering units of the upper body, and in terms of reduction of operating and recovery time and improving patient outcome, we combine the upper arm lift with breast reshaping and the upper-lateral thoracic lift as an integrated treatment in appropriate cases. Using the combination technique, a continuous approach is performed from the medial submammary fold via an anterior and posterior axillary incision line distally to the elbow. In this regard, the circumferential vectors eliminate the upper breast and lower scapular rolls and a horizontal tension to the central zone over the vertebral column is ensured (Fig. 17.3).
< div class='tao-gold-member'>


Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


