14 Electrosurgery
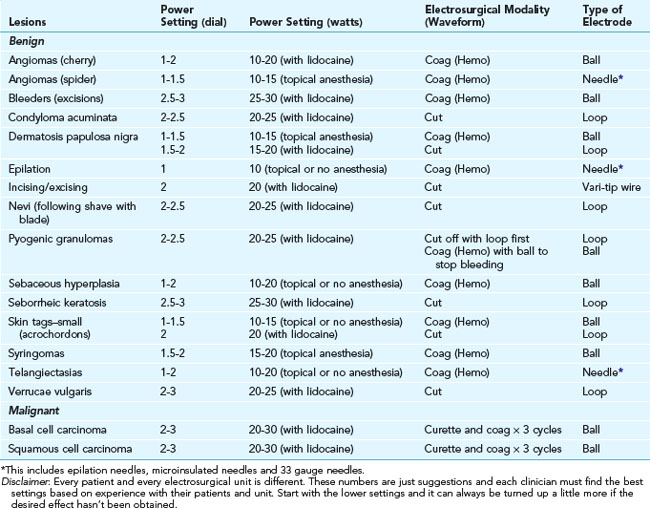
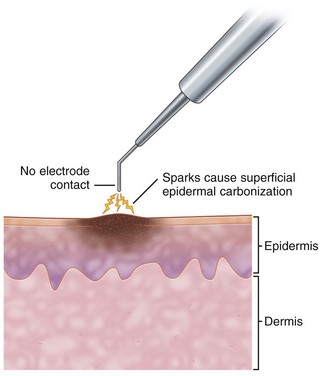
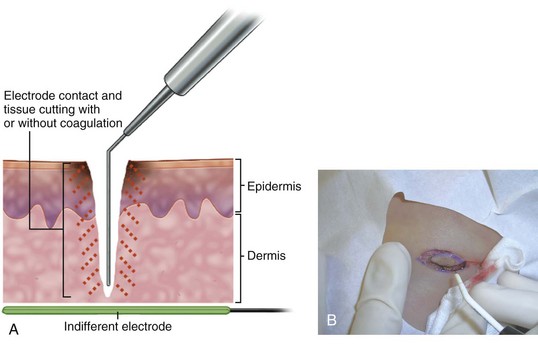
The major electrosurgical functions include fulguration, electrodesiccation, electrocoagulation, and electrosection (cutting). In fulguration, the electrode is held away from the skin so that there is a sparking to the surface (such as happens with lightning). In fact, the term fulguration comes from the Latin term fulgur, which means “lightning.” Fulguration produces a high-intensity but more shallow level of tissue destruction (Figure 14-1). With electrodesiccation, the active electrode touches or is inserted into skin to produce deeper tissue destruction (Figure 14-2). Epilation is a type of desiccation in which a fine-wire electrode is inserted into a hair follicle to literally “cook it.” Electrocoagulation is used to stop bleeding in deep and superficial surgery (Figure 14-3). In electrosection, the unit is set so the electrode cuts tissue (Figure 14-4). The higher the unit’s operating electrical frequency (not to be confused with power), the less tissue damage is left behind when using the cutting function.
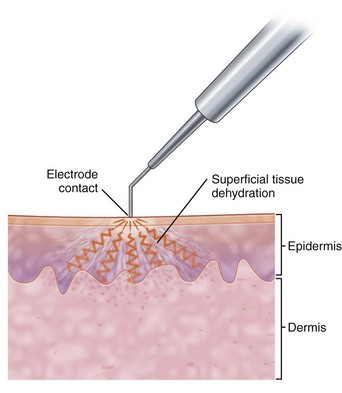
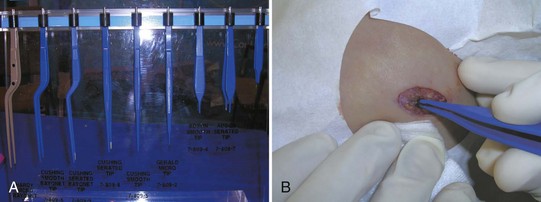
Current can be applied either in a unipolar or bipolar fashion. The majority of electrosurgical units (ESUs) are unipolar. Unipolar refers to the fact that the current enters a site at the point of the electrode and passes through the body to a grounding plate to complete the circuit. With bipolar applications, the current travels from one point of the electrode, through the tissue, to another point of the electrode (e.g., with fine forceps, from point to point). No grounding plate is needed for this type of use. This reduces possible complications from burns at unwanted sites where the current can exit. It also reduces complications with pacemakers. The bipolar units are ideal to control bleeding since forceps can pinpoint and grasp a bleeder. When the current is applied, only the tissue between the tips of the forceps is affected (Figure 14-5).
Disadvantages of Electrosurgery
Electrosurgery Versus Cryosurgery
There may be a risk of developing human papilloma virus (HPV) in the respiratory tract from inhaling the plume (smoke) from an HPV lesion as it is being treated.1–3 Intact HPV DNA has been isolated from the plume of verrucae that were treated with electrosurgery and lasers. Therefore, it is prudent for all physicians to use a smoke evacuator while performing laser and electrosurgical treatment of verrucae and other viral lesions. (See Safety Measures with Electrosurgery, p. 167.) Unfortunately, evidence is insufficient to measure the magnitude of these risks. These personal risks, however, may be one factor used to determine the physician’s choice of therapy for viral lesions.
One disadvantage of cryotherapy over electrosurgery is that with cryosurgery the final result cannot be seen immediately, and there is more subjective judgment involved in performing the treatment. However, the degree of damage can be estimated accurately with more experience and by following certain guidelines (see Chapter 15). Cryosurgery also causes more postoperative swelling, which may be uncomfortable for the patient but is only a transient phenomenon.
Electrosurgery Versus Laser
Laser is an acronym for light amplified by stimulated emission of radiation. Laser technology uses focused light energy to affect cells. Many types of lasers are available to perform different functions (see Chapters 26 through 30). Electrosurgery is less expensive than laser surgery but is more limited in utility. The standard electrosurgical units are a fraction of the cost of a laser (as low as $1000 to 4000 compared to laser units costing $30,000 to $200,000). Most physicians face the choice of referring a patient for laser surgery versus doing electrosurgery in their own office. As with electrosurgery, the CO2 laser may be used to cut, coagulate, and ablate (destroy) tissue. It is most often used in the office for resurfacing procedures, such as in the treatment of rhytids (wrinkles) and skin surface irregularities; pigmentation; and small vessels. The pulsed dye laser or a similar yellow-light laser is unequivocally better than electrosurgery for treating large hemangiomas and maximizing the cosmetic result. These lasers are used very effectively to treat port-wine hemangiomas. Visible-light lasers obtain better cosmetic results when treating most other vascular lesions, such as angiomas and telangiectasias. They offer much less chance of scarring.
Equipment
Thermal Pencil/Battery Cautery
An inexpensive thermal “pencil” cautery (Figure 14-6) is a useful device to have for small skin lesions. They are also used to occlude the cut ends of the vasa when doing a vasectomy. This disposable device consists of two penlight batteries in a housing connected to a wire filament that heats up when activated. Reusable models are also available with disposable tips. These battery cautery units can be a useful tool for treatment around the eyes and on patients with pacemakers. The devices come in high- and low-temperature varieties; low-temperature devices are preferred in skin surgery.

Electrosurgical Units
Basic Electrosurgical Units (Noncutting, Lower Frequency)
High-Frequency Units (up to 4 MHz)
Dual-Frequency Units (Unipolar 4 MHz and Bipolar 1.7 MHz)
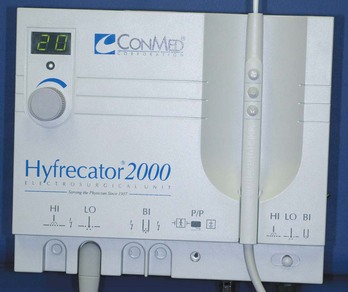
FIGURE 14-7 The Hyfrecator 2000 from the ConMed Corporation is a commonly used electrosurgical unit in the office.

Accessories
Hyfrecator


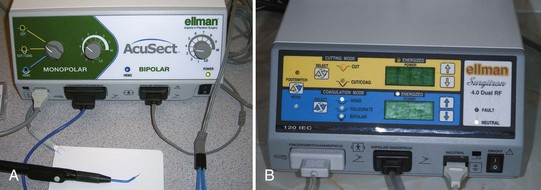
Ellman Surgitron Units
FIGURE 14-12 An assortment of medical electrodes for single use may be purchased from Ellman for use with the Surgitron.




Contraindications
Electrosurgical Techniques: General Principles
Power Setting
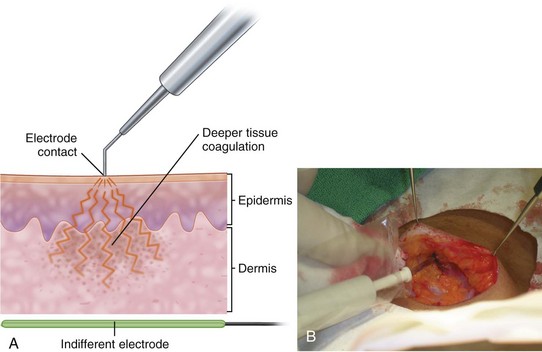
Every electrosurgical unit is different, and the desired setting will vary for each model, procedure, lesion, or patient. Even two supposedly identical electrosurgical models may require different settings. Therefore, the setting levels provided are only starting points (Tables 14-1 to 14-3 and Box 14-1). The basic principle for setting the correct power output is to start low and increase the power until the desired outcome (destruction, coagulation, or cutting) is achieved. For ablation/destruction, the tissue should bubble or turn gray. Keep in mind that destruction of tissue below the visible area of treatment can occur. The power setting for coagulation is generally higher than the setting needed for tissue destruction. A rule of thumb is to use the lowest power setting that accomplishes a given result so as to achieve cosmetically acceptable outcomes. It helps to moisten the tissue to provide better contact and allow a lower power setting.
TABLE 14-1 Range of Power Settings with the Hyfrecator 2000
Lesions | Power Setting (watts on low) | Type of Electrode |
|---|---|---|
| Benign | ||
| Angiomas (cherry) | 2–2.5 | Sharp or dull |
| Angiomas (spider) | 2–2.5 | Sharp or needle |
| Condyloma acuminata | 12–18 | Dull |
| Dermatosis papulosa nigra | 2–2.5 | Dull or sharp |
| Pyogenic granulomas | 16–20 or switch to high | Dull |
| Sebaceous hyperplasia | 2–2.5 | Dull |
| Seborrheic keratosis | 10–14 | Dull |
| Skin tags (acrochordons) | 2–2.5 | Sharp |
| Syringomas | 2–2.5 | Sharp |
| Telangiectasias | 2–2.5 | Sharp or needle |
| Verrucae vulgaris | 12–18 | Dull |
| Verrucae plana | 12–18 | Sharp or dull |
| Malignant | ||
| Basal cell carcinoma | 16–20 | Dull |
| Squamous cell carcinoma | 16–20 | Dull |
Disclaimer: Every patient and every electrosurgical unit is different. These numbers are just suggestions and each clinician must find the best settings based on experience with their patients and unit.
TABLE 14-2 Approximate Range of Power settings with Radio-Frequency Surgery (Using Dual-Frequency Ellman Surgitron)
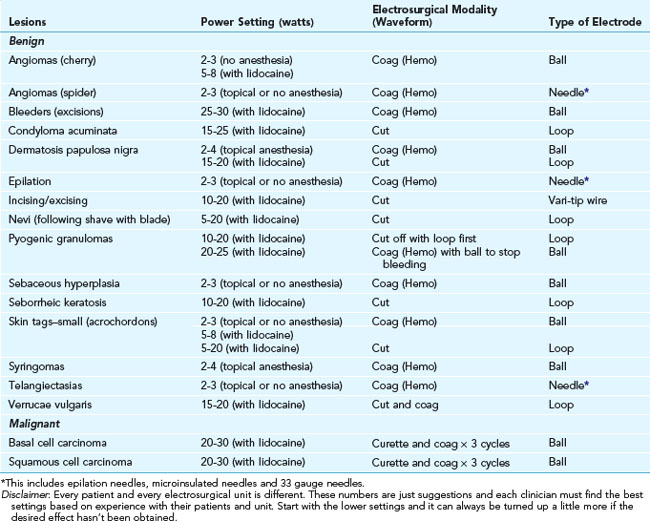
TABLE 14-3 Approximate Range of Power Settings with Radio-Frequency Surgery (Using Ellman Surgitron FFPF EMC)