This article describes a method of performing a dual nerve transfer procedure and provides illustrative cases for analysis and discussion. Clinical indications, technical pearls, and pitfalls are discussed. Dual nerve transfer for facial reanimation efficiently combines the strengths of the hypoglossal and masseteric nerve transfers and builds on existing nerve transfer techniques.
Key points
- •
Two commonly used nerve transfer procedures in facial reanimation are facial nerve-to-hypoglossal nerve and masseteric nerve–to–facial nerve transfers.
- •
Facial nerve-to-hypoglossal nerve transfer yields improvement in resting facial symmetry but minimal excursion of the oral commissure during smile. Masseteric nerve–to–facial nerve transfers improve smile but resting facial symmetry may not be successfully restored.
- •
Dual nerve transfer efficiently combines transfer of both the masseteric and hypoglossal nerves in a single surgery to improve smile and facial symmetry at rest.
Video content accompanies this article at http://www.facialplastic.theclinics.com .
Introduction
Facial paralysis has a negative impact on both appearance and communication The surgical options for facial reanimation following facial paralysis are dynamic and evolving, but nerve transfers increasingly are utilized for facial reanimation and generally are recognized as superior to stand-alone cross-facial nerve grafts. In this setting, nerve transfer involves coaptation of a regional cranial motor nerve to the nonfunctional facial nerve. The 2 most commonly performed nerve transfers in facial reanimation surgery utilize the hypoglossal and masseteric nerves as regional donors. The hypoglossal nerve–to–facial nerve transfer yields improvement in resting facial symmetry; however, this procedure offers minimal excursion of the oral commissure during smile. The masseteric transfer, conversely, provides significant smile restoration but resting facial symmetry may not be restored as successfully in some patients.
In an attempt to restore both oral commissure elevation and improve facial symmetry at rest, the senior author (JPP) recently described a combination of these 2 procedures. The dual nerve transfer for facial paralysis pairs the strengths of regional transfer of both the masseteric and hypoglossal nerves in a single surgery. This article describes the surgical technique and perioperative considerations for this relatively new procedure.
Patient selection criteria and preoperative assessment
Candidates for the dual nerve transfer procedure have irreversible and complete facial paralysis of a duration of 2 years or less with intact ipsilateral hypoglossal and masseteric donor nerves on clinical examination. If recovery of facial nerve function is uncertain, then electrodiagnostic testing at either 6 months or 12 months after onset of complete paralysis is performed. Given the use of the hypoglossal nerve, patients with clinically apparent dysphagia or aspiration are not offered treatment via this technique. It should be emphasized clearly that this technique of hypoglossal nerve–to–facial nerve transfer requires complete transection of the nonfunctional facial nerve; therefore, this procedure is reserved for patients who have no prospect for subsequent meaningful recovery of their injured facial nerve without intervention.
In patients with a history of vestibular schwannoma, radiographic assessment of the temporal bone is mandatory. The facial nerve is transected near the second genu. For this reason, surgical access to this region of the nerve must be assured radiographically. Presence of fat grafts that extend into the mastoid or other postsurgical changes from approaches to the lateral skull base must be noted.
Before and after surgery, patients undergo routine clinical assessment that includes the Facial Clinimetric Evaluation (FaCE) questionnaire and Electronic Facial Assessment by Computer Evaluation (eFACE). The FaCE questionnaire is a disease-specific patient-reported quality-of-life measure used to assess facial impairment and disability in patients with facial paralysis. It contains 15 statements, each associated with a 5-item Likert scale. Participants select the most appropriate response to prompts, with 1 corresponding to the lowest and 5 to the highest function, used to measure patients’ perceptions of specific aspects of their facial impairment and disability. These statements subsequently are grouped into 6 independent domains: social function, facial movement, facial comfort, oral function, eye comfort, and lacrimal control. The overall score is a composite of all domains. Using a specific formula that has been described previously, a score from 0 (worst) to 100 (best) is calculated. The FaCE questionnaire is a validated instrument with excellent internal consistency and test-retest reliability.
The eFACE is a clinician-graded tool that uses 15 visual analog scale scores to evaluate 3 parameters of functional facial function: static symmetry, dynamic movement, and synkinesis. Higher scores in each domain and the total composite score correlate with higher facial function. This assessment tool has been validated as a video-based scoring metric and has high intrarater and interrater reliability. All patients undergoing surgical treatment of facial paralysis are analyzed with these 2 instruments.
Surgical technique
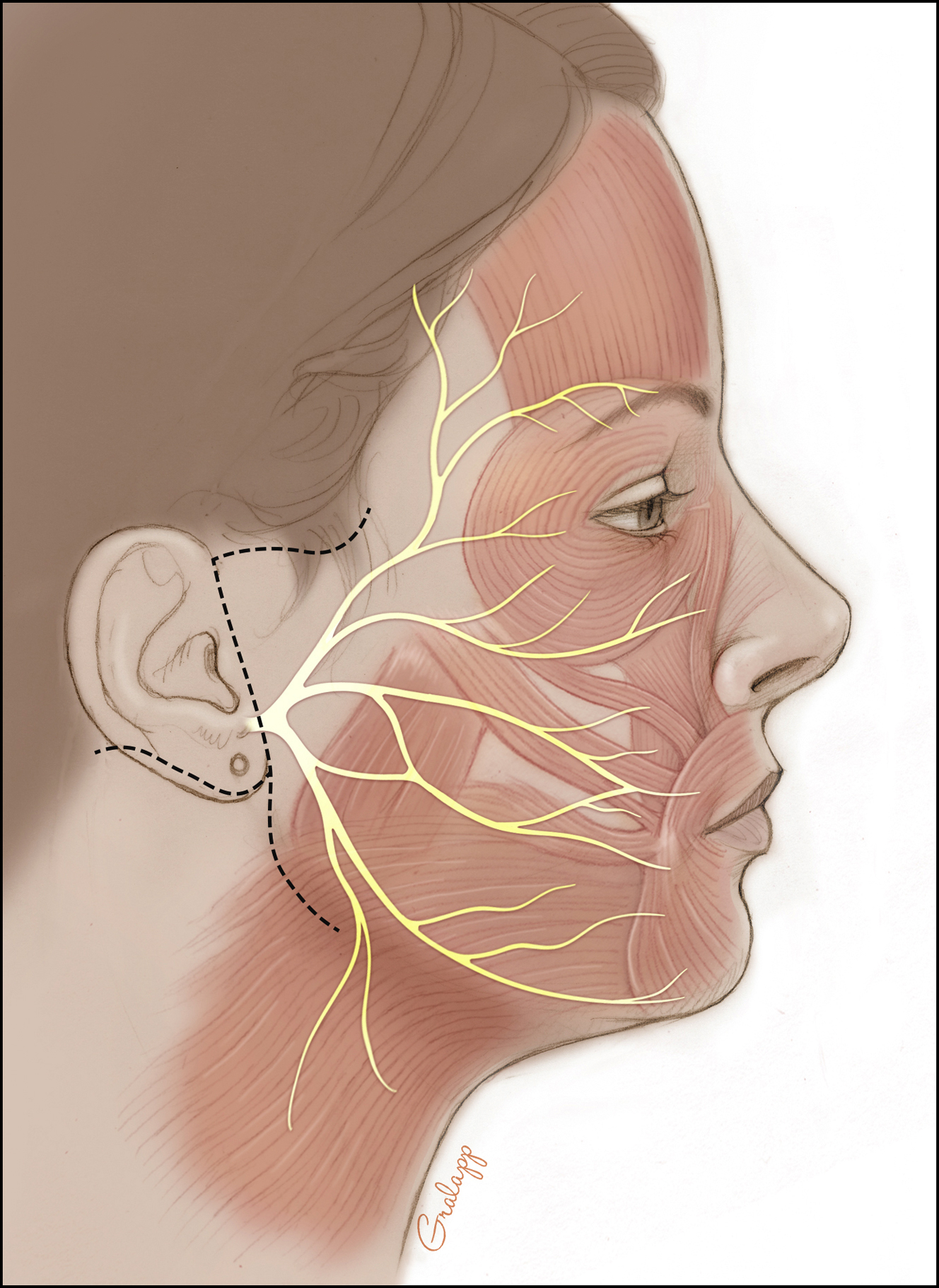
Dual nerve transfer is a 2-team surgery in most cases, involving both facial plastic surgery and otologic surgery. Incisions, therefore, include a modified rhytidectomy incision that is extended into both the inframandibular and postauricular creases to provide simultaneous access to the mastoid region, masseteric nerve, and hypoglossal nerve ( Fig. 1 ). Blood supply to the auricle is maintained through both an intact superior cutaneous bridge and deep soft tissue connections both preauricularly and via the vascular supply of the ear canal. Coaptation of the second genu of the facial nerve to the hypoglossal nerve is performed first. A mastoidectomy is performed, the facial nerve is decompressed from the fallopian canal, and the nerve is transected near the second genu ( Fig. 2 ). The portion of the facial nerve distal to the transection point then is mobilized into the neck. Effective transposition is achieved by dividing the posterior auricular branch of the facial nerve and the fibrous periosteal attachments at the superficial aspect of the stylomastoid foramen. Without these steps, the intratemporal facial nerve may not have sufficient length to reach the hypoglossal nerve. , In some cases, the posterior belly of the digastric muscle also is divided. The ipsilateral hypoglossal nerve is identified deep to the posterior belly of the digastric muscle. A partial neurotomy is made in the superior aspect of the nerve. The transected facial nerve then is transposed to the hypoglossal nerve and an end-to-side coaptation is completed with 3 interrupted 9-0 nylon sutures, followed by administration of thrombin gel around the coaptation site ( Fig. 3 ). All nerve sutures are placed while visualized with an operating microscope.
Related posts:
 Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
Temporalis Tendon Transfer Versus Gracilis Free Muscle Transfer
 Modified Selective Neurectomy
Modified Selective Neurectomy
 Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
Lessons from Gracilis Free Tissue Transfer for Facial Paralysis
 Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
Reinnervation with Selective Nerve Grafting from Multiple Donor Nerves
 Treating Nasal Valve Collapse in Facial Paralysis
Treating Nasal Valve Collapse in Facial Paralysis
 Facial Reanimation and Reconstruction of the Radical Parotidectomy
Facial Reanimation and Reconstruction of the Radical Parotidectomy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


