(1)
Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil
6.1 Synonyms
Granuloma inguinale, granuloma venereum, granuloma inguinale tropicum, granuloma contagiosum, ulcerating granuloma, ulcerating sclerosing granuloma, chronic venereal ulcer, granuloma donovani.
6.2 Concept
Progressive disease characterized by ulcerating granulomatous lesions that are painless and self-inoculable. This disease mostly affects the skin and mucous membranes of the genital, perineal and inguinal regions.
6.3 Incubation Period
Widely variable, from 3 days to 6 months.
6.4 Etiological Agent
The etiological agent of donovanosis used to be known as Donovania and then came to be known as Calymmatobacterium granulomatis. In a well-founded study published in 1913, professors Aragão and Vianna [1], who were studying patients in the city of Rio de Janeiro, proposed the name Calymmatobacterium granulomatis. In 1999, Carter et al. [2] used molecular methods and phylogenetic similarities to propose the reclassification of the agent as Klebsiella granulomatis comb. nov. However, Kharsamy et al. [3], while studying 16S rRNA gene sequencing found a similarity of approximately 95% for the Klebsiella and Enterobacter genera. Therefore, they concluded that C. granulomatis was a unique organism. This organism is a Gram-negative facultative aerobic bacteria, apparently an intestinal saprophyte and possibly opportunistic, which depending on individual susceptibility or bacteriophage action can penetrate the tegument and cause the disease.
6.5 Clinical Manifestations (Figs. 6.1–6.14)
The disease has a range of symptoms, including ulcerative lesions with a bright red granulomatous base that easily bleeds, with hypertrophic or flat borders, which may be ulcerovegetative or with elephantiasis and that may develop necrosis. A varying number of these ulcers can be observed and may sometimes be multiple, and they are chronic and usually not associated with regional lymphadenopathy. Extragential manifestations occur in 6% of cases and systemic dissemination via the blood causing damage to the bone and liver is rare.
6.6 Laboratory Diagnosis
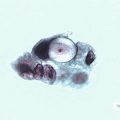
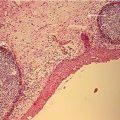
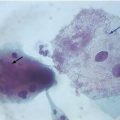
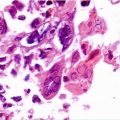
Identification of C. granulomatis via Donovan bodies (Figs. 6.15–6.17) is most easily carried out using cytological smears and lesion biopsies stained by Wright, Papanicolaou, Giemsa or Leishman technique. These are found inside the cytoplasm of histiocytes and macrophages in the form of encapsulated cocobacilli, which are pleomorphic with rounded edges and become brightly stained with appearance of a safety pin. It is recommended that one swab be taken from the center of the lesion and another from one of the recently developed borders. This procedure is also recommended for biopsies (using the Hematoxylin-Eosin staining technique), which must also contain healthy skin. To the Giemsa staining technique the slide should be air dried, and when using the Wright, Leishman or Papanicolaou techniques the slide should be fixed using alcohol or another cytological fixative agent. A specific kit should be used for analysis of swabs taken from lesions with liquid based cytology. It is true that liquid based cytology can make cellular characteristics easier to observe. However, we do not know of any comparative studies between conventional cytology and liquid based cytology. The culture for this type of bacteria is difficult in terms of its nutritional requirements. Genital lesions over 30 days old, particularly those that have not healed, require histopathological testing. Other diagnostic methods such as PCR and serological screening have still not been standardized or made commercially available.
6.7 Evaluation of Laboratory Methods
Exam | Sensitivity % | Specificity % |
|---|---|---|
Swabs and biopsy | 40–50 | <50 |
Cultures and PCR of swabs taken from lesions are unfortunately not available in routine medical practice, even in developed countries. However, in many cases it is possible to collect and store material for later molecular biology testing at a microbiological research laboratory | ||
6.8 Treatment and Cure
The protocols set out by the Centers for Disease Control and the European guidelines for the management of donovanosis recommend the same medication. Treatment time is 3 weeks or until clinical cure has been achieved for all proposed regimens.
CDC (2010) | EURO (2010) | |
|---|---|---|
Regimen | • Oral doxycycline 100 mg,12/12 h | • Oral azithromycin 1 g, once a week |
• Oral azithromycin 1 g, once a week | • Oral azithromycin 500 mg, once a day | |
• Oral ciprofloxacin 750 mg, 12/12 h | • Oral Sulfamethoxazole/trimethoprim (800 mg and 160 mg), 12/12 h | |
• Oral erythromycin 500 mg, 6/6 h | • Oral doxycycline 100 mg, 12/12 h | |
• Oral Sulfamethoxazole/trimethoprim (800 mg and 160 mg), 12/12 h | • Oral erythromycin 500 mg, 6/6 h | |
• Gentamicin 1 mg/kg, IV, 8/8 h | ||
Pregnant women | • Oral erythromycin 500 mg, 6/6 h | • Oral erythromycin 500 mg, 6/6 h |
• Consider adding a parenteral aminoglycoside (gentamicin, for example) | • Oral azithromycin 1 g, once a week | |
Observations | • Consider adding an aminoglycoside (for example, gentamicin 1 mg/kg, IV, 8/8 h) for any regimen if an improvement is not seen in the first days of treatment | • Children: Azithromycin 20 mg/kg |
Other therapeutic regimen have been used successfully, all of which for 3 weeks or until complete cure has been achieved:
Oral ciprofloxacin 500 mg, 12/12 h (contraindicated for pregnant women, breastfeeding mothers and children);
Oral thiamphenicol 500 mg, 12/12 h.
Control of cure is predominantly clinical.
6.9 Complications
Long-lasting lesions can suffer from secondary infections leading to deformations, mutilations and fistulas. In women this may lead to obstructive lymphatic obstructions that can develop into elephantiasis forms. Although rare, extragenital disease can occurr, generally resulting from a primary genital lesions and affecting the bones and other areas, especially in immunosuppressed patients. The development of squamous cell carcinoma in chronic ulcers is well documented, with a high incidence in patients with donovanosis.
6.10 Differential Diagnosis
Syphilis, soft chancre, cutaneous tuberculosis, ulcerative neoplasia, American tegumentary leishmaniasis and other ulcerative and granulomatous cutaneous disease.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


