Abstract
Sudoriferous glands, i.e. sweat glands, lie within the dermis and subcutaneous fat. There are two types of sweat glands: eccrine and apocrine. Eccrine sweat glands represent the vast majority of sweat glands within human skin whereas apocrine glands have a much more limited distribution. The most commonly used classification system for hyperhidrosis divides it into primary and secondary types. Other classification systems separate hyperhidrosis into categories based on the source of the neural impulses that drive it: cortical (emotional), hypothalamic (thermoregulatory), medullary (gustatory), spinal cord, and local axon reflexes. Treatment options for axillary and volar hyperhidrosis include topical aluminum chloride, oral agents (anticholinergics, α- or β-adrenergic blockers, α 2 -adrenergic agonists), onabotulinumtoxinA, iontophoresis, biofeedback therapy, and surgical procedures. Causes of hypo- and anhidrosis include central or neuropathic disruption of neural impulses, sweat gland abnormalities, and medications. In addition to abnormal function, specific sweat gland disorders (e.g. miliaria, neutrophilic eccrine hidradenitis) are primarily related to obstruction or inflammation.
Keywords:
eccrine gland, apocrine gland, sweat gland, sweat, hyperhidrosis, hypohidrosis, anhidrosis, miliaria, neutrophilic eccrine hidradenitis, Fox–Fordyce disease, chromhidrosis, bromhidrosis, granulosis rubra nasi, keratolysis exfoliative, idiopathic palmoplantar hidradenitis
Sweat Glands
Eccrine Sweat Glands
- ▪
2–5 million eccrine glands are unevenly distributed over the skin surface
- ▪
In healthy individuals, eccrine sweat is 99% water
- ▪
Sweating is a reflex sympathetic autonomic function mediated by cholinergic neurons
Although there are 2–5 million eccrine glands distributed within the skin, none are found on the clitoris, glans penis, labia minora, external auditory canal, or lips. Eccrine glands are separate from the apocrine-pilosebaceous apparatus, and by dermoscopy, eccrine ductal orifices can be seen along the dermatoglyphic ridges of the palms and soles. The average healthy adult can produce over 0.5 liters of sweat per hour, 99% of which is water. Athletes or those acclimatized to hot environments can produce up to 3–4 liters per hour . Physically fit or acclimatized persons initiate sweating earlier and conserve sodium, chloride, and other electrolytes more efficiently. Thermoregulatory control is similar in men and women and diminishes only slightly with age .
Sweating is a reflex function controlled primarily by the sympathetic nervous system. These nerves are anatomically sympathetic but functionally cholinergic, i.e. acetylcholine, rather than norepinephrine, is the principal terminal neurotransmitter. Neural impulses for sweating (sudomotor impulses) travel from the anterior hypothalamus via the reticulospinal tracts to the appropriate level in the spinal cord, out through the rami communicantes to autonomic ganglia, and then within sympathetic cholinergic neurons to the secretory cells of the eccrine glands. Adrenergic innervation of eccrine glands has also been demonstrated, but is not believed to be physiologically important . In addition, the sweat glands, via a direct effect on the secretory cells, respond to certain drugs (e.g. cholinergic agonists) as well as to the local application of heat.
Apocrine Sweat Glands
In humans, apocrine sweat glands are confined to the eyelids (Moll’s glands), external auditory meatus, axillae, areola and nipple, periumbilical region, and anogenital region, in particular the mons pubis, labia minora, prepuce, scrotum, and perianal area. At five months gestation, apocrine glands are distributed all over the body, whereas in a full-term neonate they are limited to the above sites. In non-primate mammals, apocrine sweat glands are widely distributed but they also open into the pilosebaceous unit.
Apocrine secretion is a slow, usually continuous process analogous to milk formation in the mammary gland. The secretory product is an oily fluid composed of lipids, proteins, and sex hormones. At or near the skin surface, it mixes with sebum derived from the sebaceous gland that empties into the same pilosebaceous unit.
Hyperhidrosis
- ▪
Excessive sweating
- ▪
Primary hyperhidrosis is the most common type, typically affecting the palms, soles, and/or axillae
- ▪
Secondary hyperhidrosis is due to an underlying condition (e.g. genetic syndrome, infection, tumor) or medication and may be localized or generalized
Primary Hyperhidrosis
▪ Primary focal hyperhidrosis
- ▪
Main sites are volar (palms, soles) and axillary skin; the face may also be involved
- ▪
Hyperhidrosis arises from increased cortical stimulation and occurs only during waking hours (diurnal)
- ▪
Patients are otherwise healthy
- ▪
Up to 80% of affected individuals have a family history of hyperhidrosis
| CRITERIA FOR THE DIAGNOSIS OF PRIMARY HYPERHIDROSIS |
|
Intense emotion or stress can elicit sweating in anyone. It occurs most often on the palms, soles, or axillae and can also affect the face ( Fig. 39.1 ), especially the forehead and the cutaneous upper lip. The post-orgasmic sweating observed with sexual activity may also derive from emotional stimulation .

Clinically significant primary hyperhidrosis occurs in two major patterns: volar (palmoplantar) and axillary, which can coexist , but usually one of the two sites predominates. The onset of volar hyperhidrosis is often during childhood, whereas axillary hyperhidrosis typically develops at or soon after puberty. Primary hyperhidrosis is seen in both cold and warm environments. A chronic and unremitting course is characteristic, with little or no variation in association with age, disease, or hormonal status.
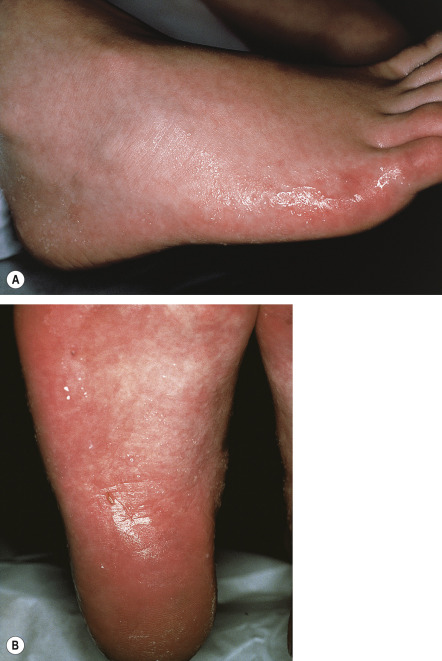
Volar hyperhidrosis is the most common form of primary hyperhidrosis ( Fig. 39.2 ), affecting ~50–60% of patients . The entire palm and sole, as well as the lateral aspects, tips and distal dorsal skin of the fingers, display sweating. It can clearly have an impact on quality of life.
Axillary hyperhidrosis is the second most common form of primary hyperhidrosis, affecting 30–50% of patients . The right axilla usually produces more sweat than the left (60 : 40). Exceptionally, one axilla may be hyperhidrotic while the opposite axilla is hypohidrotic or virtually anhidrotic. Odor (axillary bromhidrosis) is usually absent; the excessive quantities of eccrine sweat presumably rinse away or dilute odorogenic apocrine sweat droplets and bacteria.
Secondary Hyperhidrosis
Secondary hyperhidrosis is caused by or associated with another systemic disorder. It may be localized or generalized. There are many causes, which can be divided into categories based on the source of the neural impulse driving the response: cortical, hypothalamic, medullary, spinal cord, or local. A number of medications may also be associated with hyperhidrosis ( Table 39.2 ).
| DRUGS THAT CAN STIMULATE ECCRINE SWEATING | |
|---|---|
| Direct-acting cholinomimetic agents | |
|
|
| Cholinesterase inhibitors | |
|
|
| Adrenomimetic agents | |
|
|
| Antidiabetic (hypoglycemic) agents | |
|
|
| CNS stimulants | |
|
|
| Antidepressants | |
| |
| Antipsychotics | |
| Antipyretics | |
| Opioids | |
| Other drugs | |
* Increased sweating is infrequently observed at pharmacologic doses but represents a sign of overdose.
† Combination of MAOIs (which include linezolid as well as antidepressants) with drugs such as tricyclics, SSRIs, certain opioids and tryptophan can result in the serotonin syndrome, which is characterized by mental status changes, autonomic hyperactivity (including hyperhidrosis), and neuromuscular abnormalities.
Disorders associated with cortical (emotional) hyperhidrosis
- ▪
Several disorders of cornification and other genodermatoses affecting palmoplantar skin are associated with volar hyperhidrosis
- ▪
Patients with hereditary autonomic neuropathies can also exhibit cortical hyperhidrosis
| CAUSES OF CORTICAL (STRESS/EMOTIONAL) HYPERHIDROSIS |
| Primary hyperhidrosis |
| Secondary hyperhidrosis |
| Disorders of cornification |
|
| Other genodermatoses |
|
| Hereditary sensory and autonomic neuropathies (HSANs) † |
|
Hypothalamic (thermoregulatory) hyperhidrosis
- ▪
Due to elevated body temperature (e.g. acute febrile illness, lymphoma, chronic infection) or direct hypothalamic stimuli (e.g. pheochromocytoma, medications, toxins)
- ▪
May be nocturnal (night sweats) or diurnal
Febrile illnesses are among the most common pathologic states that cause hypothalamic sweating. At the height of the fever, notably with temperatures of 39–40°C (102–104°F) or above, sweating is absent, the apparent result of inhibition of the hypothalamic center for sweating. With defervescence, sweating characteristically ensues. Lymphomas and chronic infections (e.g. tuberculosis) can present with episodic thermoregulatory sweating, which may be described as “night sweats” (that actually follow unperceived mild febrile pulses).
Generalized sweating of hypothalamic origin can also be seen in a number of metabolic and endocrine disorders ( Table 39.4 ). Patients with diabetes mellitus may exhibit hypohidrosis as well as various forms of hyperhidrosis. For example, hyperhidrosis is a characteristic sign of insulin-induced hypoglycemia (but not diabetic ketoacidosis), and compensatory hyperhidrosis of the trunk can develop in the setting of diabetic neuropathy affecting the extremities (see below). In addition, diabetics may exhibit gustatory hyperhidrosis, primarily of the face and neck. Troublesome sweating of the scalp can also be seen in poorly controlled diabetics, and, with regulation of the hyperglycemia, the hyperhidrosis often improves.
| CAUSES OF HYPOTHALAMIC HYPERHIDROSIS | ||||||
|---|---|---|---|---|---|---|
| Infection | Tumors | Endocrine/metabolic | Vasomotor | Neurologic | Drugs/toxins | Miscellaneous |
|
|
| ||||
* Via release of catecholamines (pheochromocytoma) and serotonin (carcinoid tumors, usually metastatic; see Ch. 106 ).
† Patients have sympathetic activation, with impaired vasodilatory responses to heating but preserved sweating.
‡ Also associated with cortical hyperhidrosis.
§ Referred to as Hines–Bannick syndrome or, when associated with agenesis of the corpus callosum, Shapiro syndrome.
∥ Autosomal recessive condition caused by mutations in the genes encoding cytokine receptor-like factor-1 and cardiotrophin-like cytokine factor-1; additional features include facial dysmorphism, flexion deformities (elbows, fingers), and scoliosis.
¶ Compensatory hyperhidrosis is also a feature of Ross syndrome (segmental anhidrosis, generalized areflexia and tonic pupils).
Disorders with vasomotor instability, such as Raynaud phenomenon, autoimmune connective tissue diseases, frostbite and other cold injuries, and reflex sympathetic dystrophy, may be associated with excessive sweating because of disturbed autonomic function . A synchronous discharge of vasoconstrictor and sudomotor impulses evokes a “cold sweat”, usually of the hands and feet, producing macerated, soggy wet, violaceous skin known as symmetrical lividity.
Cerebral cortex lesions, such as a tumor, abscess or cerebrovascular accident, may be associated with a contralateral hyperhidrosis due to an impairment of the inhibitory cortical influence that normally regulates hypothalamic sudomotor activity . Hypothalamic sweating is also observed in Parkinson disease and occurs as the “sweating sickness” following encephalitis. Harlequin syndrome, characterized by unilateral flushing and hyperhidrosis in association with contralateral anhidrosis, may be due to peripheral or central nervous system (CNS) abnormalities .
Episodic release of catecholamines from pheochromocytomas directly stimulates the hypothalamus and may elicit sweating . Exposures to toxins and medications can also lead to hypothalamic hyperhidrosis, and a number of drugs that act on the CNS have increased sweating as a potential side effect (see Table 39.2 ). Additional causes of hypothalamic hyperhidrosis are presented in Table 39.4 .
Pressure and postural hyperhidrosis may be due to hypothalamic or possibly cortical stimulation. With changes in posture or the application of pressure to one side of the supine individual, a variety of sweating patterns have been described, such as lateral hyperhidrosis, horizontal hemihidrosis, and crossed hemihidrosis. Idiopathic localized unilateral hyperhidrosis of the face and neck or forearm has been reported as an episodic disorder triggered by heat, emotional, or gustatory stimuli .
Medullary (gustatory) hyperhidrosis
- ▪
Taste receptors in the mouth are the source of the afferent impulses that stimulate sweating
- ▪
Physiologic medullary hyperhidrosis is most commonly triggered by spicy foods, alcohol, and citrus fruits
- ▪
Pathologic medullary hyperhidrosis occurs when disrupted nerves for sweat aberrantly connect with nerves for salivation; this can be caused by local injury to, or disease of, the parotid gland (Frey syndrome), trauma to the sympathetic trunk, and CNS disorders (e.g. encephalitis, syringomyelia)
Physiologic medullary hyperhidrosis
Any food or drink that stimulates the taste buds may induce sweating in normal individuals, particularly of the face. This is thought to occur via a variant reflex arc in which afferent impulses from taste bud receptors travel via the glossopharyngeal nerve to nuclei within the medulla oblongata (hence the term “medullary” hyperhidrosis), but lead to provocation of sweating rather than (or in addition to) the usual response of salivation. A few minutes after ingestion of a stimulating food or beverage, sweating and erythema are seen most commonly on the upper cutaneous lip or cheeks. It may be unilateral or bilateral and may be brief or persist as long as the stimulating food or beverage is ingested. Associated vasodilation localized to the areas of sweating causes the erythema, which may be faint. Spicy or sharp-tasting foods and beverages, such as citrus fruits, alcohol and condiments, may elicit the reaction. It is most common in children and young adults and in warmer environments. A familial tendency has been described . There are no other concurrent local or systemic signs or symptoms. A variant of gustatory hyperhidrosis can occur on the face in diabetics. Unusual types of gustatory hyperhidrosis involving the scalp and the knee have also been described and support the concept of a central medullary mechanism for these sweating responses .
Pathologic medullary hyperhidrosis
This disorder arises after disruption of nerves. During healing, nerve fibers mediating sweating aberrantly connect to nerves that mediate salivation. Impulses in parasympathetic fibers normally supplying the salivary glands are now misdirected to the sweat glands. As a result, salivary stimulation elicits sweating. Of note, thermal sweating in the areas of affected skin is reduced.
The parotid form appears weeks to months following surgery, trauma, or other disorder (e.g. abscess, herpes zoster) affecting the parotid gland. These patients experience vasodilation and sweating on the cheek and adjacent neck when salivary stimulation is induced by eating, drinking, or even chewing ( Fig. 39.3 ). Sweating most often occurs in the distribution of the auriculotemporal nerve; at times there is also unilateral localized pain .

Auriculotemporal syndrome (Frey syndrome) is common after parotid surgery, developing in 40% or more of patients, although many are not aware of it. It can also occur during infancy (frequently as a consequence of trauma to the parotid region in a forceps-assisted delivery), presenting with gustatory flushing, but usually no obvious sweating, that is often erroneously attributed to food allergy. Another variant of gustatory hyperhidrosis is the chorda tympani syndrome in which salivary stimuli to the submandibular gland induce sweating on the chin and lower jaw line.
Patients with cluster headaches can have sympathetic deficits that result in impaired thermoregulatory sweating on the affected side of the forehead. In addition, ipsilateral hyperhidrosis and flushing may occur together with excessive lacrimation during headache attacks. This is due to misdirection of parasympathetic fibers, which normally supply the lacrimal glands, to sweat glands and blood vessels. Patients with Raeder syndrome (Horner syndrome [ptosis, meiosis ± anhidrosis] plus unilateral temporofrontal headaches and pain) may also have excessive supraorbital sweating (lacrimal sweating).
Any condition that injures the vagus nerve and sympathetic trunk, as they lie close together in the thorax, may cause a pathologic medullary hyperhidrosis ( Table 39.5 ). Cholinergic fibers from the vagus nerve sprout into the adjacent sympathetic trunk during the healing process and can result in a gustatory hyperhidrosis with sweating on the face, neck, and portions of the trunk and upper extremities.
| OTHER CAUSES OF SECONDARY HYPERHIDROSIS | |||
|---|---|---|---|
| Medullary (gustatory) | Spinal cord | Axon reflex | Abnormal blood vessels or eccrine glands (non-neural) |
|
|
|
|
In patients with syringomyelia or encephalitis, gustatory hyperhidrosis is occasionally seen on the face and upper trunk. It involves the glossopharyngeal and vagus nerves. Disturbances in the brainstem apparently lead to transposition of the central medullary nuclei for salivation and sweating. There is no peripheral crossing of sympathetic and parasympathetic nerve fibers as is seen in other forms of pathologic gustatory hyperhidrosis.
Spinal (cord transection) sweating
- ▪
Spinal disorders may result in a lack of thermal sweating below the injury as well as unusual patterns of hyperhidrosis
- ▪
Mass reflex sweating may occur around the injured level
Autonomic dysreflexia
- ▪
Direct stimulation (e.g. electrical, physical, or drug-induced) of a sympathetic axon can cause sweating
- ▪
May be seen with inflammatory skin diseases
Direct stimulation of a cutaneous sympathetic axon with electrical and physical impulses or injections of drugs with nicotine-like effects on autonomic ganglia can induce sweating in an area ~4 cm in diameter . Mediators from inflammatory skin conditions (e.g. psoriasis, dermatitis) can also elicit localized hyperhidrosis. Substance P and a number of other mediators, including kinins, dopamine, prostaglandins, angiotensin and adenine, may be involved .
Compensatory hyperhidrosis
- ▪
Anhidrosis in one area may cause hyperhidrosis in another
- ▪
Miliaria, diabetic neuropathy, and sympathectomy are well-known causes
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


