Abstract
The description, diagnosis, and management of skull base cerebrospinal fluid (CSF) leaks has a long, controversial history dating back to the first report of this entity in the 17th century. With regards to demographics, in those sustaining closed head injuries (CHI), 10%–20% of patients have a basilar skull fracture and 1%–3% have CSF leaks. Importantly, 52% of those with skull base CSF leaks will note resolution of their leak within 5 days of onset. As such, those with simple, linear, nondisplaced skull base fractures with CSF leakage are more likely to halt with conservative management and can be appropriately managed in this fashion. However, given that those with persistent skull base CSF leaks have a 20%–50% chance of experiencing an adverse infectious event (meningitis, extra-axial empyema, and/or brain abscess[es]), for those CSF leaks persisting beyond 5 days or more acute scenarios with large, displaced osseous skull base defects operative intervention (either via an endoscopic transnasal approach or a more traditional transcranial approach) is warranted. The use of prophylactic antibiotics in the pre- and/or perioperative setting has been on the decline due to the lack of rigorous evidence supporting its use and fears of inducing antibiotic resistance or favoring more invasive/aggressive organisms. Of final note, regardless of the modality of treatment, one must be vigilant for the possibility of CSF leak recurrence in both short- and long-term follow-up. As such, continuity of care should be ensured and patients and their families should be counseled thoroughly about the signs and symptoms of CSF leaks and meningitis that can occur.
Keywords
cerebrospinal fluid leak, skull base fractures, traumatic brain injury
Background
History
The description, diagnosis, and management of skull base cerebrospinal fluid (CSF) leaks has a long, controversial history dating back to the first report of this entity in the 17th century by Bidloo. In his report, the Dutch surgeon described a case of profuse posttraumatic CSF rhinorrhea that resulted in the death of his patient 7 months later from meningitis. Then, in the late 1800s, Chiari was the first to document the link between CSF rhinorrhea and traumatic injuries to the paranasal sinuses with concomitant pneumocephalus. These early cases highlighted the end result modern practitioners aim to prevent and the impetus behind the increasingly sophisticated methods and techniques used to treat this condition.
The early 1900s saw further classification of skull base CSF leaks and the first descriptions of the surgical repair of dural defects causing these leaks. Using his experience with both closed and penetrating brain injuries, Hugh Cairns in a 1937 paper classified CSF rhinorrhea into four categories that are still applicable today (see Table 1.6.1 ). In addition, Walter Dandy visualized and repaired a dural tear at the base of the skull with tensor fascia lata in the same time frame.
|
|
|
|
Military conflicts since World War I have revealed CSF leaks to be harbingers of significant morbidity and mortality. In the Iran–Iraq War, CSF leaks were an independent variable contributing to deep central nervous system (CNS) infections in military missile head wounds in a regression model. Additionally, as modern protective gear and helmets have improved, the incidence of individuals’ sustaining penetrating injuries to the skull base via transfrontal, transorbital, and transfacial routes have only increased. Finally, the high energy imparted by modern penetrating and nonpenetrating blast injuries creates closed head and paranasal sinus injuries classically associated with CSF rhinorrhea and otorrhea in the civilian population.
Demographics and Associated Injuries
In the general population, head trauma is the major cause of morbidity and mortality between the ages of 1 and 44, with approximately 50,000 Americans dying annually from traumatic brain injury (TBI). Among those sustaining closed head injuries (CHI), 10%–20% have a basilar skull fracture and 1%–3% have CSF leaks. Additionally, approximately 1.7% of individuals with blunt mechanism facial fractures will sustain basilar skull fractures and 9.7% will have cervical spine fractures. Among those experiencing CSF leaks, over 80% present with CSF rhinorrhea and the other 20% with otorrhea. Also, between 20% and 50% of patients with CSF leaks will develop CNS infections if left untreated with no resolution of their leak. Of note, for those sustaining basilar skull fractures, a CSF leak does not have to be present for meningitis to occur and said event can be quite remote from its antecedent trauma.
Surgical Anatomy
The anterior skull base is formed by the confluence of the frontal, ethmoid, and sphenoid bones with their corresponding paranasal sinuses being the most common sources of CSF rhinorrhea given their intimate relationship with the basal dura of the frontal lobes (see Fig. 1.6.1 ).
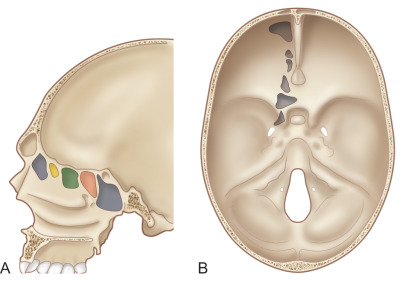
Positioned at the apex of the nasal cavity, the frontal sinus derives from the extension of the frontal recess into the frontal bones. The sinus begins to pneumatize at 2 years of age and is usually apparent radiographically beginning at 6 years of age, reaching an average volume of approximately 3.5 cm 3 . Its mucosal drainage via the nasofrontal outflow tract into the semilunar hiatus is critically important in the clinical decision making regarding fractures of this complex.
Typically present at birth, the ethmoid sinuses reach their average volume of approximately 4.5 cm 3 by 16 years of age and are classically divided into anterior, middle, and posterior divisions. Pneumatization of the sphenoid sinus is usually apparent by 1 year of age and reaches its average full volume of 3.5 cm 3 by the age of 15, with a growth spurt occurring between 6 and 10 years of age.
Clinical Presentation
History, Clinical, and Laboratory Assessment
One must consider several important historical findings in those with skull base fractures and concomitant CSF leaks. In addition to the timing and mechanism of injury, one should also note any reports of loss of consciousness, seizure activity, or periods of hypoxia or hypotension as these can independently affect prognosis and subsequent decision making. While severe craniomaxillofacial trauma can be dramatic at first glance, one should always remember the basic tenets of trauma care and resuscitation. ATLS guidelines and protocol should be followed on presentation and no further neurosurgical treatment planning should commence until it is certain that the patient is stable from a cardiopulmonary standpoint. During this time, one may perform a neurological examination (to attain a Glasgow Coma Score [GCS]) prior to intubation (if possible) and stop any arterial hemorrhage from scalp or facial wounds by simple closure with staples or sutures. In addition to standard trauma protocols utilizing the placement of rigid cervical collars and universal spine precautions, those in which there is a significant concern for cervical spine injury should undergo a full American Spinal Injury Association (ASIA) exam to fully describe and characterize the completeness and neurological level of any potential spinal cord injury. Finally, all cooperative patients should undergo cranial nerve testing to rule out an orbital apex syndrome or optic nerve injury.
The clinical and physical signs of those with skull base CSF leaks typically mimic those with all basilar skull fractures (mastoid ecchymosis [Battle’s sign], periorbital ecchymosis [raccoon eyes], etc.). When found clinically and/or radiographically, one should have a high index of suspicion for CSF leakage and perform a detailed physical examination as such. Aside from the obvious signs of CSF rhino/otorrhea, one should attempt to examine the posterior oropharynx for the “glistening” sight of CSF drainage. In addition, CSF accumulation behind the tympanic membrane should be examined for using an otoscope. In the obtunded or sedated patient, endoscopy may be utilized to examine the paranasal sinuses, skull base, posterior oropharynx, and Eustachian tube in a more detailed manner for CSF drainage. Additionally, examination of the orbit may reveal CSF leakage or a pulsatile globe due to an orbital roof fracture that may have a corresponding dural tear. In awake patients, additional symptoms such as positional headaches, the sensation of postnasal drip, a “salty” taste in the back of the mouth, or a feeling of fluid/fullness in the ear should be identified.
For cases in which the clinical diagnosis of CSF rhino or otorrhea is uncertain, certain laboratory findings can assist in confirming what may be a presumptive diagnosis. Glucose and protein levels have been used in the past, utilizing normative values to help establish whether the fluid in question is in fact CSF. One should use caution with this method alone though, as these values can vary in the presence of infection/meningitis and in those with diabetes, which can affect the interpretation of results. Beta-2 transferrin (beta-2 trf), the desialated isoform of transferrin, is only present in CSF and has a sensitivity and specificity of 84% and 100% (respectively) in the diagnosis of CSF leakage. However, most assays require between 2 mL and 5 mL of fluid for successful analysis, which may be problematic for those with low-flow/volume or intermittent CSF leakage (which account for the majority of cases with clinical/diagnostic uncertainty). Additionally, the laboratory assay for beta-2 transferrin is not readily available at all hospital/clinical laboratories and as such may take several days to weeks to process at outside facilities. As a result, laboratory analysis of fluid concerning for CSF leakage serves a limited role and should be used as only one of the factors that seasoned clinicians use in diagnosis.
Radiological Evaluation
Computed Tomography (CT)
In modern practice, fine-cut (less than 1 mm) CT scans of the face, sinuses, and head in the axial, sagittal, and coronal planes are the best way to examine for the skull base and sinus fractures typically associated with CSF leakage and pneumocephalus. With regards to the frontal sinus, the status of both the anterior and posterior walls in addition to the patency of the nasofrontal ducts should be assessed. Given the multiplicity and thin bony architecture of the ethmoid sinuses, fractures can often be difficult to detect. However, the presence of ethmoid opacification on CT, air cells appearing to communicate with the intracranial compartment, or frank pneumocephalus are harbingers of injury to this complex.
Basilar skull injuries affecting the middle cranial fossa typically result in either longitudinal or transverse fracture patterns of the petrous pyramid. Of note, longitudinal fractures are more likely to result in CSF otorrhea given their tendency to involve the posterior portion of the external auditory canal and the tegmen tympani. One should also examine for any involvement of the carotid canal, facial canal, cochlea, and semicircular canals in these particular fractures.
The injection of intrathecal contrast in conjunction with CT imaging as specified above is another method to more precisely localize the potential site(s) of CSF leakage. Additionally, the use of intrathecal fluorescein can be of great assistance in localizing the site of CSF leak either pre- or intraoperatively utilizing endoscopic assistance.
Magnetic Resonance Imaging (MRI)
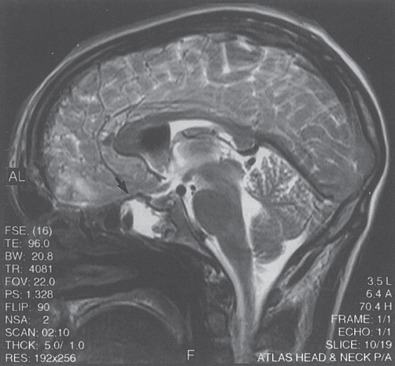
For cases in which clinical uncertainty exists regarding actual CSF leakage or where further anatomic clarification of potential leak sites would be beneficial further imaging studies may be indicated on a case-by-case basis. Multiplanar fine-cut T2-weighted MR imaging can reveal CSF accumulation into particular paranasal sinuses and even the site of potential dural tears or pseudo-meningoceles (see Fig. 1.6.2 ). This information can be invaluable for clinical decision making and planning the surgical approach (open vs. endoscopic) one takes for a particular case.
Nuclear Medicine (NM) Studies
When the clinical signs, symptoms, and imaging work-up to date are equivocal for the absence or presence of a skull base CSF leak, nuclear medicine studies can assist in basic diagnosis. By performing an intrathecal injection of metrizamide with nasal pledgets placed beforehand, technicians can then examine for the presence (or absence) of the tracer at various intervals (usually up to 24 hours) after the injection. This modality is typically reserved more for an absolute determination of CSF leakage when other modalities have failed to yield adequate diagnostic information.
Considerations in the Initial Management of Skull Base CSF Leaks
Timeframe and Mechanism of Injury
When considering the aggressiveness, modality, and timing of treatment with regards to traumatic skull base CSF leaks, one must take into account the timeframe and underlying mechanism of CSF liquorrhea. The shearing forces typically associated with the acceleration/deceleration mechanisms of closed head injuries usually create linear/simple defects in the paranasal sinuses and surrounding dura. Early CSF leaks associated with these injuries may be more likely to heal with conservative or nonoperative management as presented further in this chapter. It is also important to remember that skull base CSF leaks may present in a delayed manner (more than one week post-injury) as brain parenchymal and sinus mucosal swelling abates after an initial injury.
Medical Stabilization and Management of Concomitant Intracranial Injuries
Once initial cardiopulmonary stabilization and resuscitation has occurred and diagnostic imaging has been obtained, life-threatening intracranial injuries such as acute subdural or epidural hematomas should be searched for. Additionally, the presence of traumatic subarachnoid blood, parenchymal contusions, or diffuse cerebral edema resulting in cisternal effacement should be noted as these may affect the timing and modality of subsequent CSF leak treatment. If any of the above are present, they should be treated appropriately and the patient started on 7 days of antiepileptic medications.
If a patient has an acute cranial neurosurgical emergency with a concomitant skull base CSF leak, it is at the provider’s discretion as to whether the two conditions can be managed in a single operative procedure. In an ideal setting this would always be the case, however it is rarely so. Regardless, surgeons should always consider the possibility of future approaches in those at risk of skull base CSF leaks and design their incisions such that they do not preclude adequate access to the paranasal sinuses or sufficient autograft (split-thickness calvarium, pericranium, or temporalis fascia/muscle) for skull base/dural repair if needed at a later point.
Intracranial Pressure Monitoring and CSF Diversion
Of those with acute posttraumatic skull base CSF leaks, approximately 52% will cease spontaneously with a short period (5 days) of observation. For those with persistent skull base CSF leaks after observation or acute high volume leaks in the setting of severe paranasal sinus and skull base trauma, a principle tenet of management is that of CSF diversion. This period of drainage allows for maximal scar tissue to form at the site(s) of dural lacerations to lessen the chance of recurrence. One case series of 24 patients with anterior fossa skull base CSF leaks found that a period (5–7 days) of CSF diversion halted 70% of such leaks.
CSF diversion can occur by multiple means to include ventricular drainage, lumbar drainage, or serial lumbar punctures. For those with intracranial injuries and neurological exams (Glasgow Coma Scale [GCS] <8) in which intracranial pressure monitoring would be useful, the placement of an intraventricular catheter (IVC) would serve to measure and treat intracranial pressure elevations and divert CSF from sites of skull base dural tears.
For those cases in which intracranial pressure monitoring is not indicated, the authors prefer lumbar drainage as the first choice for CSF diversion in skull base CSF leaks. Less ideally, serial lumbar punctures are an option for those with limited resources or supplies.
Nonoperative Management of CSF Leaks and Potential Controversies
As mentioned previously, approximately 52% of skull base CSF leaks will halt spontaneously within 5 days of their onset. As such, observation of those with relatively simple, linear, noncomminuted, and nondepressed skull base/paranasal sinus fractures with a concomitant CSF leak may be observed closely for a short period of time. At the senior author’s institution, standard protocol consists of head elevation to greater than 30 degrees at all times, CSF diversion of some form in all patients, and fluid restriction. In addition, supplemental oxygen administration via face mask or nasal cannula is strictly avoided (if needed, a face tent may be used) and nose-blowing (as well as the use of straws for drinking) is prohibited. No prophylactic antibiotics are administered.
With regards to the use of prophylactic antibiotics for those with skull base CSF leaks, a Cochrane review published in 2011 using five randomized controlled trials (RCTs) and 17 non-RCTs found no evidence to support the use of prophylactic antibiotics for those will skull base CSF leaks. As a result, this practice, once controversial, has been steadily on the decline. In fact, only 14% of respondents of a 2014 survey indicated they administer prophylactic antibiotics. Most clinicians cited concerns over inducing bacterial resistance or altering nasopharyngeal flora to more invasive organisms.
However, it is widely known that safe and effective vaccines exist against the three most common pathogens of bacterial meningitis ( Streptococcus pneumoniae , Neisseria meningitides , Haemophilus influenzae ) with primary and secondary antibody responses taking between 5 and 10 days and 21 days, respectively. Given the lifelong immunity imparted by these vaccinations, some individuals and societies are beginning to recommend administration to all patients with confirmed skull base CSF leaks. At current writing though, more study is needed to examine the effect this intervention may have on those who do and do not develop bacterial meningitis after sustaining a skull base CSF leak.
The use of acetazolamide to decrease CSF production in those with skull base or paranasal sinus injuries has been advocated by some given its ability to decrease CSF production by up to 48%. However, a recent RCT found no significant effect on the duration of CSF leakage in those administered acetazolamide compared to the control group and a significantly higher incidence of medical complications (metabolic acidosis and hypokalemia) in the experimental group.
Surgical Indications and Timing
Penetrating head injuries, in particular those associated with high-velocity projectiles (such as military-grade weaponry) create complex sinus, skull base, and dural injuries that if associated with high-volume CSF leakage are less likely to respond to nonoperative management and CSF diversion. As such, early (within 24–48 hours of presentation) operative coordination and planning may be warranted to prevent subsequent infectious sequelae.
For those with blunt mechanism injuries and persistent CSF rhino- or otorrhea failing to resolve after 5–7 days of observation and subsequent CSF diversion, operative intervention is warranted and planning should proceed as presented below. Additionally, in those whose leaks halt with nonoperative management, one must be vigilant for the possibility of recurrence in both the short and long term. As such, clinical follow-up should be ensured and patients and their families should be counseled thoroughly about the signs and symptoms of CSF leaks and meningitis.
Related posts:
 Frontal Bone and Frontal Sinus Injuries
Frontal Bone and Frontal Sinus Injuries
 Le Fort Fractures
Le Fort Fractures
 Secondary Reconstruction of Facial Soft Tissue Injury and Defects
Secondary Reconstruction of Facial Soft Tissue Injury and Defects
 Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Secondary Microvascular Reconstruction of the Traumatic Facial Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


