This article provides an update on histopathologic studies of different types of melanocytic lesions, such as site-specific nevi, “Spark’s” nevi, nevi during pregnancy, and atypical dermal melanocytic proliferation, including pigmented epithelioid melanocytoma, proliferating nodules, and atypical Spitzoid tumor. Special-site nevi, such as those appearing on the breast and genital region, generally have more cytologic and architectural atypia. Melanocytic proliferations generally do not change during pregnancy, contrary to earlier observations. Atypical dermal melanocytic proliferations are difficult to diagnose and usually have a better outcome after adequate treatment, including wide local skin excision with or without sentinel lymph node resection.
- •
Special site nevi such as those on the breast and genitalia tend to have more cytologic and architectural atypia but can be considered benign changes.
- •
The histopathology of melanocytic proliferations during pregnancy does not appear to differ significantly.
- •
Atypical dermal melanocytic proliferations are difficult to diagnose and tend to have a better outcome after adequate treatment.
- •
Additional histopathologic studies along with longer clinical follow-up are required to determine if atypical dermal melanocytic proliferations and special site nevi will behave as low grade malignant neoplasms or benign neoplasms.
Site-specific nevi (dysplastic nevi or not?)
Normal skin biopsies from different anatomic locations from 97 patients in Australia were examined for the distribution of melanocytes using an immunohistochemical stain for tyrosinase-related protein 1. This study showed that overall melanocyte density decreases with age, and the density is highest on the back, shoulder, and limbs. In addition, patients with more nevi had a higher density of melanocytes. Hair color, eye color, and freckling did not have an impact on the density of melanocytes. Another study of 506 Australian children showed that the highest number of nevi were on the arms, neck, and face. Girls had more nevi on the lower leg and thigh than boys. These simple and eloquent studies show that the density of melanocytes and nevi differ, suggesting that the biology of melanocytes from different locations and genders may vary. Reasoning would follow that melanocytic proliferations from different locations and genders also will probably be different.
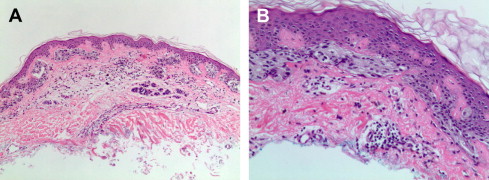
Hosler and colleagues recently wrote an excellent review on nevi with site-related atypia., categorizing them into 4 groups: acral, genital, special-site, and conjunctival. And they review on nevi with site-related atypia, the special-site category included breast, flexural, scalp, and auricular sites. These special-site nevi can have more cytologic atypia and architectural disorder than other sites ( Fig. 1 ). For example, 101 breast nevi showed more dermal fibroplasia, cytologic atypia, and intraepidermal melanocytes compared with 97 other nevi. Similar studies from other special sites have also been reported. However, these studies do not address whether these atypical nevi really represent completely benign nevi or whether dysplastic nevi occur more frequently at these sites. Recognition is important to ensure that melanoma is not overdiagnosed. However, in some instances, whether atypia is attributed to site-specific changes is not straightforward, and some dermatopathologists might still recommended complete conservative removal.
Related posts:
 Cytogenetic and Mutational Analyses of Melanocytic Tumors
Cytogenetic and Mutational Analyses of Melanocytic Tumors
 Fibrous and Fibrohistiocytic Neoplasms
Fibrous and Fibrohistiocytic Neoplasms
 Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Update on Vascular Neoplasms
Current Understanding of Cutaneous Lymphoma
Direct Immunofluorescence Testing in the Diagnosis of Immunobullous Disease, Collagen Vascular Disease, and Vascular Injury Syndromes
New Directions in Dermatopathology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


