Abstract
The chapter provides the reader with a basis for the treatment of dental and dentoalveolar injuries. This includes anatomy of the dentition, periodontium, and associated structures. A foundation is offered for examining and diagnosing dentoalveolar trauma and classification systems are reviewed. Current treatment recommendations for dentoalveolar injuries are reviewed, including live patient videos of a reduction of a tooth with splint placement and arch bar placement for a dentoalveolar fracture.
Keywords
dental trauma, dentoalveolar fractures, tooth fractures, tooth displacement
Background
Dentoalveolar trauma represents a significant proportion of facial injuries. Treatment of dentoalveolar trauma has been documented as early as the era of Hippocrates, who described the use of dental splinting with bridal wires. Although many advances have occurred, the basic principles of fixation of loose teeth or bony segments to allow for hard and soft tissue healing are still paramount.
The incidence and prevalence of injuries to the dentoalveolar complex are difficult to determine. Dentoalveolar injuries are often treated in an office setting and largely underreported. Across the globe, dental injury affects nearly one-third of preschool children in the primary dentition. Trauma to the teeth due to a fall is the most common facial injury in this age group. Subsequently, 25% of children in the mixed dentition sustain dental trauma most commonly due to sports injuries. Lastly, 25% of adults sustain a traumatic injury to permanent teeth. There is a large variance in the incidence of injuries depending on race, socioeconomic status, age, sex, geographic location, anatomic factors (e.g. class II dental relationship) and medical conditions (seizures, gait or balance disturbances). These injuries can occur in isolation or in association with craniofacial fractures and/or orthopedic injuries. Fortunately, the overall incidence of craniofacial injuries is decreasing in developed regions due to advances in motor vehicle safety, traffic laws, reduction in intoxicated driving, and improved safety equipment for athletes (e.g. mouth guards and face masks). Injuries as a result of interpersonal violence, falls during daily life activities, and sports-related injuries have become more common than those from motor vehicle collisions.
The mechanism of dentoalveolar injury is either direct trauma to the teeth or secondary to a blow to the chin resulting in the mandibular dentition being forced into the maxillary dentition. Direct injury most commonly affects the maxillary central incisors, which protrude beyond the other teeth. Predisposing conditions include class II malocclusion (overjet >4 mm), labially inclined central incisors, and lip incompetence. Children are more likely to sustain damage to the underlying periodontal structures (i.e., luxation or avulsion of teeth) than adults, who are more likely to sustain tooth or alveolar bone fractures. The presence of the developing secondary dentition, smaller less pneumatized maxillary sinuses, and less dense bone make the pediatric alveolar bone more pliable and resistant to fracture.
Surgical Anatomy
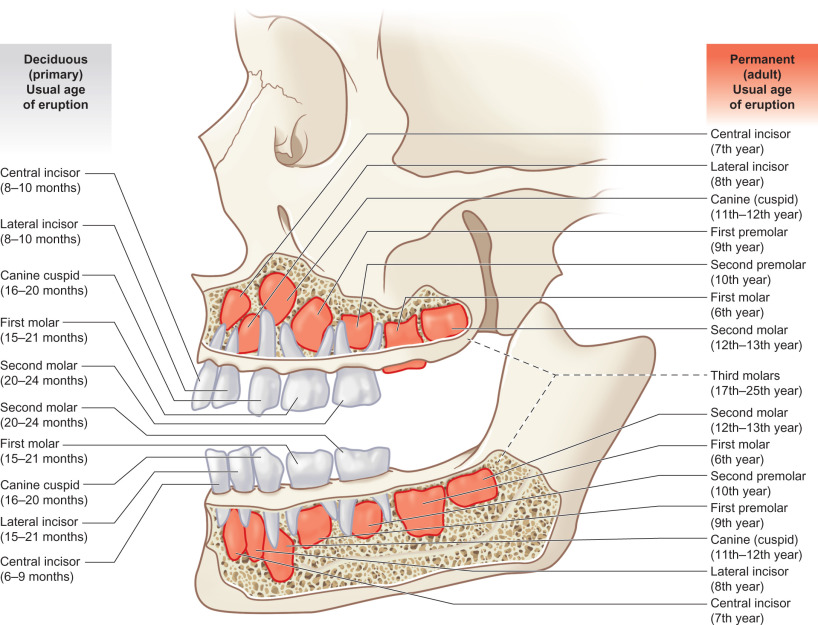
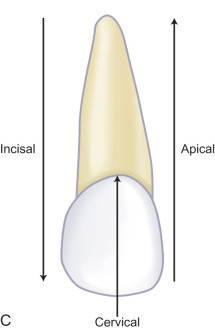
When considering the anatomy of dentoalveolar injuries, distinction must be made between primary and adult dentition as well as between teeth and the periodontium. A complete deciduous dentition includes two primary molars, a canine, and lateral and central incisors in each quadrant for a total of 20 teeth. The adult dentition includes three molars, two premolars, a canine and lateral and central incisors in each quadrant for a total of 32 teeth. At age 6, the adult first molars erupt posterior to the primary second molars, starting the ‘mixed dentition’ phase. A well-defined pattern of primary tooth exfoliation and adult tooth eruption ensues leaving one with mixed dentition until the last primary tooth exfoliates around 12 years of age ( Fig. 1.18.1 ).
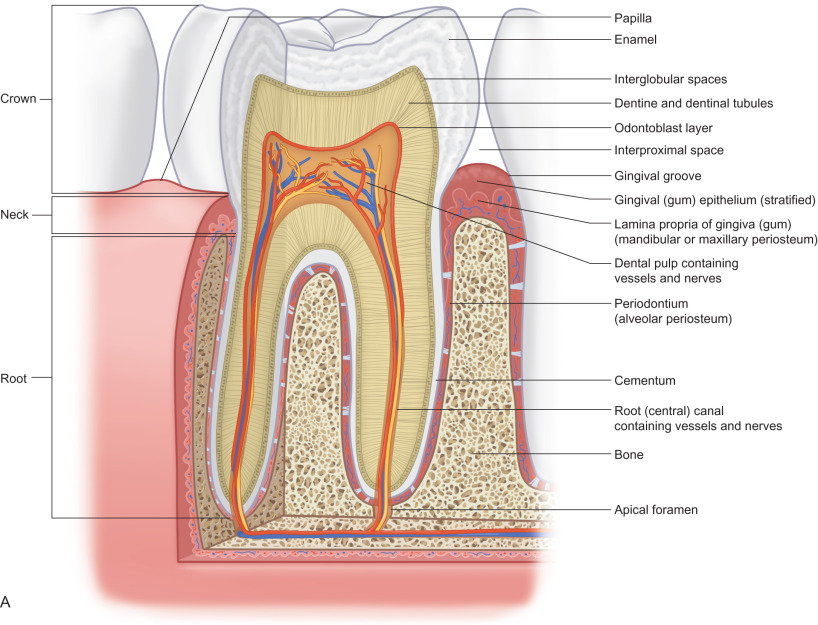
All teeth are composed of enamel, dentin, dental pulp, and cementum ( Fig. 1.18.2 ). The periodontium is the structures that support the teeth, including the periodontal ligament, alveolar bone, and the overlying gingiva. As the name suggests, dentoalveolar injuries involve either or both dental structures along with alveolar bone. The term is oversimplified as injuries can include fractures through enamel, dentin, and exposure of the pulpal tissues and typically involve disruption of the periodontal ligament and lacerations of the overlying gingival mucosa.
Dental Anatomy
Enamel , dentin , and cementum are the calcified structures of the dentition made up of 96%, 70%, and 50% inorganic mineral components, respectively. Enamel, the hardest substance in the human body, is the outer surface of the crown of a tooth, with high compressive strength and brittle nature. It is acellular and lacks reparative capacity. Cementum is the outer layer of the root, extending from the cementoenamel junction (CEJ) to the root apex. Cementoblasts remain on the surface and are entrapped as new matrix is formed. The cells, deriving nutrition from the adjacent vascularized periodontal ligament, provide ability for some self-repair after injury. Beneath enamel and cementum lies dentin, with a low compressive but high tensile strength due to greater organic content, providing support for the overlying crown. The internal wall of dentin is lined with odontoblasts with cytoplasmic extensions spanning the length of the dentinal layer through dentinal tubules that can respond to external insults with additional dentin formation over time. Dental fractures extending to this layer tend to be associated with hypersensitivity, likely due to hydrodynamic forces through the dentinal tubules.
Pulpal tissue is the neurovascular bundle of the tooth contained within the pulp chamber and root canals. It comprises the central portion of the tooth and is easily visible on dental films. In primary and new permanent teeth there are extensions of the pulp towards the occlusal surface called pulp horns increasing the likelihood of pulp exposure in pediatric dental fractures.
Periodontal Anatomy
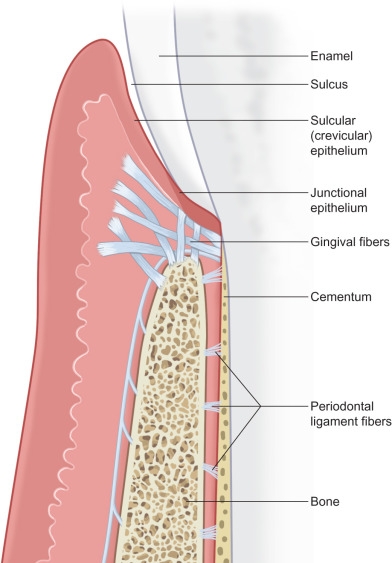
The periodontal ligament (PDL, Fig. 1.18.3 ) is a set of connective tissue fibers that secure the tooth to the adjacent alveolar bone. It provides for physiologic mobility and helps support the tooth against compressive forces through its insertion into cementum (via Sharpey’s fibers). It is seen on dental radiographs and orthopantomograms as the radiolucent line between the tooth and the cortical margin of the adjacent alveolar bone known as the lamina dura (see Fig. 1.18.8 ). The PDL is highly vascular, providing blood supply to the adjacent cementum. Osteoblasts and cementoblasts are within the PDL, allowing for reparation of alveolar bone and cementum. The viability of the PDL and associated cells after trauma is important in the prognosis of the injured tooth. Loss of the PDL leads to ankylosis of the tooth to the bone or external resorption of the tooth.
Alveolar bone supports teeth in the maxilla and mandible. It consists of buccal/facial and lingual/palatal cortices that surrounding trabecular bone along with a cortical alveolar lining (lamina dura) comprising the tooth socket. The cortical plates are supported by Haversian systems and are thinnest in the maxillary teeth and thickest over the posterior mandibular teeth. The status of the less-supported buccal/facial plate following injury or extraction of a tooth can determine the need for bone grafting prior to dental implant placement to replace the tooth. All measures should be taken to preserve as much alveolar bone as possible after dentoalveolar trauma.
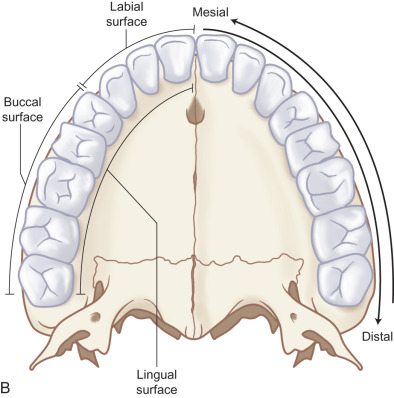
Gingiva is the soft tissue lining that overlies the alveolar bone and surrounds the dentition ( Fig. 1.18.3 ). It is made of epithelial and deeper connective tissue components. The reduced enamel epithelium surrounds an erupting tooth and forms a complex attachment at the cementoenamel junction of the tooth thereby sealing the deeper periodontal structures from the oral environment. In a healthy state there exists 1–3 mm of a gingival sulcus between the attachment of the gingiva to tooth structure and the visible portion of the tooth (free gingival margin). This mucosa immediately adjacent to the teeth is highly keratinized and tightly bound to the underlying alveolar bone. Unlike the buccal mucosa or that of the floor of the mouth it is immobile and provides protection during masticatory function. On the facial aspect of the maxilla and the facial and lingual aspects of the mandible the attached gingiva extends several millimeters and forms a junction with the unattached mucosa (mucogingival junction, Fig. 1.18.4 ). On the palatal aspect of the maxilla the mucosa remains keratinized and tightly bound to the hard palate. It is important to maintain and properly position the keratinized gingiva after dentoalveolar trauma.

Clinical Presentation
Examination of the injured face can be daunting. One should avoid focusing on the obvious injuries and perform a detailed history and systematic physical exam in a focused and efficient manner. Injuries to the teeth and supporting structures should be evaluated urgently as many injuries require diagnosis and treatment in a limited timeframe.
A complete history surrounding the injury must be obtained, including the mechanism, onset, duration, and associated symptoms. It is imperative to consider that patients with dentoalveolar trauma may have concomitant head, cervical spine or airway injury and patients should be evaluated appropriately (see Chapter 1.1 , Assessment of the patient with traumatic facial injury, for details).
A detailed dental history including previous treatments (prosthetics, gingival surgery, orthodontia) and the patient’s perception of their premorbid occlusion should be obtained. In cases of tooth avulsion, the clinician must determine how long the tooth has been avulsed, what type of medium the tooth has been stored in, and if it is a primary or permanent tooth. It is recommended to request preinjury facial photographs to determine the patient’s native occlusion, facial symmetry, and contours. If the patient has undergone orthodontic treatment, photographs and dental models should be sought to help establish the native occlusion.
A comprehensive and methodical physical exam should be performed on every patient with dentoalveolar trauma. Once appropriate interventions are performed to stabilize the patient with life-threatening injuries as part of the primary survey, the clinician performs a detailed maxillofacial examination as part of the secondary survey. In patients with bilateral mandibular fractures and tooth avulsions/fractures a detailed airway and pulmonary evaluation are also important as mandibular fractures can compromise the airway due to loss of soft tissue support and risk of aspiration of avulsed teeth or tooth fragments.
An accurate maxillofacial examination is only possible following adequate exposure, which includes cleaning the patient’s face and wound. Given the vascularity of the maxillofacial region, blood and debris from even minor soft tissue lacerations can misrepresent the severity of injury. Proper cleaning and examination of wounds may require sedation or general anesthesia to ensure patient comfort. A standard set of photographs should be obtained of patients sustaining facial trauma ( Fig. 1.18.5 ), including anterior, lateral, submental, intraoral, and wound photographs. These photos provide a baseline examination for medicolegal purposes, allow for a visual tool to describe treatment to the patient, and aid the clinician in forming the definitive treatment plan. This chapter will focus on the examination of the oral cavity and mandibular function.






Extraoral exam: Initial evaluation of the dentition should start with asking the patient to open and close their jaw. Deviation of the mandible with opening, premature occlusion (i.e., teeth hitting early preventing the remaining teeth from coming together) with shifting of the mandible, limitation in mouth opening, and pain when biting should be recognized. Next, measurements of the maximal incisal opening (MIO) and lateral excursive movements should be performed.
Intraoral soft tissue exam: A detailed and systematic soft tissue examination is then performed, starting with inspection for abrasion, ulceration, lacerations, hematoma, swelling, and pre-existing pathology. All lacerations should be carefully inspected for the presence of foreign body (e.g. dental restorations, tooth fragments, bone, or debris). Gingival lacerations should raise suspicion for dentoalveolar fractures or dental luxations. Laceration in the floor mouth should raise suspicion of salivary duct injury. The submandibular gland should be massaged to confirm expression of clear saliva from the opening of Wharton’s duct to help rule out salivary duct injury ( Fig. 1.18.6 ). Hematoma within the floor of mouth is often associated with dentoalveolar or mandibular fractures. The tonsillar pillars and uvula should also be examined for symmetry as any deviation could indicate airway compromise.

Intraoral hard tissue exam (bone): The hard tissue exam includes evaluation of the maxillary, mandibular, alveolar, and palatal bone, as well as the dentition. Fractures of the mandible or dentoalveolar segment often result in interdental step-offs, increased dental spacing, mobility of dentoalveolar segments (two or more teeth moving as a unit). More subtle findings may include crepitus, bleeding from the gingival sulcus, gingival lacerations or floor of mouth ecchymoses.
Intraoral hard tissue exam (dentition): The surgeon must first account for all preexisting teeth, teeth fragments or restorations. If there is avulsion or loss of a sizeable portion of a tooth, the fragment should be assumed to be in the oral cavity, airway, or GI tract until proven otherwise. Radiographs of the head, neck, chest, and abdomen (KUB) should be obtained to locate displaced teeth unable to be located to rule out aspiration. An understanding of the types of restorations (e.g. fixed/removable prostheses, implants, crowns, fillings, and orthodontic appliances) is useful in determining the extent of the injury and account for displacement. Be aware of indirect dental injury with forced occlusion of teeth from a superiorly directed force on the chin resulting in crown and/or root fractures of the posterior dentition.
Next, each remaining tooth and restoration should be evaluated systematically (see Classification section ). Transillumination of visible light along the long axis of the tooth can identify subtle dental injuries to enamel. Each tooth should be evaluated for mobility, both individually or along with its adjacent teeth (indicating a dentoalveolar fracture). Mobility of an individual tooth can indicate luxation of the entire tooth or a root fracture that can require dental radiographs to diagnose. The clinician should then evaluate the alignment of the dental arches. Teeth are most commonly displaced in a buccolingual direction due to the vector of trauma perpendicular to the tooth’s long axis. A tilting of the occlusal plane can indicate luxation or intrusion injuries, but may indicate maxillary or mandibular fracture. Each tooth should be tested for mobility in all dimensions with care not to avulse loose teeth or dentoalveolar segments. A commonly used mobility index is the Miller classification, in which tooth mobility is evaluated using two hard objects (e.g. two tongue depressors). If a tooth is nondisplaced but mobile, this may indicate either preexisting periodontal disease or a crown/root fracture. Dental fractures more coronally positioned generally have more mobility.
Intraoral occlusal exam: The patient is instructed to carefully bring their teeth into occlusion with the clinician evaluating the movement. Premature occlusal contacts could indicate fracture or luxation injuries. The patient is then guided into their premorbid occlusion if tolerated. This allows the clinician to determine the complexity of restoring the patient’s dentition. Interferences of the palatal cusps of the molars with a seemingly intact mandible could indicate a palatal fracture with change in the transverse width of the maxilla.
Tooth percussion and vitality testing: An injury to a tooth and periodontal ligament without displacement is referred to as a subluxation. Subluxated teeth have increased mobility or pain to percussion relative to adjacent teeth. Percussion is performed by applying a vertical or horizontal force using a blunt object (e.g. the back end of a dental mirror or tongue blade) and can determine damage to the PDL. A subluxated tooth will also have a change in the quality of sound produced by percussion from the normal sharp metallic sound to a dull resonance. Dental injuries can disrupt the neurovascular bundle at the apex of teeth. Tooth vitality testing measures the ability of the nerve fibers of the tooth to relay information to the trigeminal system. This is performed routinely by dentists and endodontists using different methods with varying sensitivity, including thermal (hot or cold), electric, pulse oximetry, and laser Doppler flowmetry ( Fig. 1.18.7 ). Within the first several weeks after dental trauma vitality testing is not reliable and is typically done after several weeks to months to determine the need for endodontic treatment for non-vital teeth.

Radiological Evaluation
The last two decades have seen a dramatic advance in head and neck imaging. The advent of digital radiographs and cone beam computed tomography (CBCT) has revolutionized the way many hospital and community-based clinicians utilize imaging. The goal of imaging is to evaluate the tooth roots, pulp canals, and periodontium for preexisting disease and traumatic injury. In children, radiographs also serve to evaluate the development of the tooth roots and location of the succedaneous tooth buds relative to injuries. Imaging can also be used post treatment to confirm tooth or bone reduction and position of hardware. This section will serve as a guide for use of different types of imaging available. The availability of imaging modalities varies widely in the emergency room setting, but most centers have facial films and computed tomography (CT).
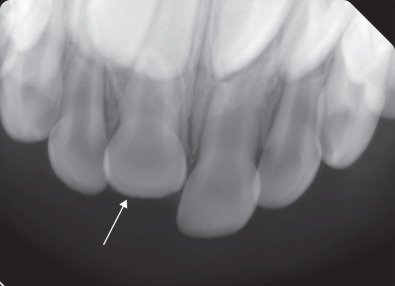
Intraoral radiographs: Intraoral radiographs are high-resolution two-dimensional radiographs that include bitewings, periapical, and occlusal film used by dentists and dental specialists. Bitewings evaluate tooth crowns and alveolar bone to detect caries and periodontal disease. They have little utility in the setting of trauma. Periapical radiographs (PA) show the crowns and roots of 1–4 teeth. They show the periodontal ligament, and alveolar bone around the tooth. Multiple angles may be needed to detect a root fracture. PA films can be used to confirm reduction following splinting of avulsed and luxated teeth by comparing the position of the tooth root to the surrounding cortical margin of the socket (lamina dura). Occlusal films are taken perpendicular to the occlusal plane of the maxilla and mandible and are larger than PAs ( Fig. 1.18.8 ). They are easier to obtain than periapical radiographs in the trauma setting as they do not require that the film or sensor be placed into the lingual or palatal tissue. They can be used to identify crown/root fractures, luxation injuries, and are useful in detection of radiopaque foreign bodies or tooth fragments in the surrounding soft tissue (e.g. floor of mouth, lips, vestibule).