Cutaneous Manifestations of Systemic Disease
OVERVIEW
Characteristic skin features can be clues to more serious underlying systemic illnesses. The cutaneous surface, nails, hair, and the mucosal surfaces, including the oral cavity, often afford clues to many underlying disorders. The skin is sometimes referred to as a “window to disease.” For example, the presence of jaundice, palmar erythema, pruritus, and spider telangiectasias points to liver disease.
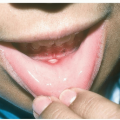
The appearance of pyoderma gangrenosum, erythema nodosum, or severe aphthous stomatitis may indicate associated inflammatory bowel disease. Periungual findings can suggest various collagen vascular disorders such as systemic lupus erythematosus, dermatomyositis, and scleroderma. By appreciating skin signs of systemic diseases, the health care provider can often lead their patient to an early diagnosis, appropriate treatment, and referral to other specialists if needed.
CUTANEOUS MANIFESTATIONS OF ENDOCRINE DISORDERS
Diabetes Mellitus-Associated Lesions
Acanthosis Nigricans
Acanthosis nigricans sometimes occurs in insulin-resistant diabetes, obesity, and in Cushing and polycystic ovary syndromes.
Velvety, hyperpigmented plaques arising most often in the axillae, groin, and the neck (Fig. 22-1; see also Figs. 10-7, 10-8, and 12-8).
Necrobiosis Lipoidica (See also LEGS)
Necrobiosis lipoidica (NL) was formerly referred to as “necrobiosis lipoidica diabeticorum” or “NLD.” Currently, the term necrobiosis lipoidica is used to encompass all patients with the same clinical lesions regardless of whether diabetes is present or not, since a minority of these patients have, or will develop, diabetes mellitus. NL has also been described in patients with sarcoidosis, inflammatory bowel disease, and in otherwise healthy patients.
When it does appear in diabetics, NL is seen more frequently in association with type 1 rather than type 2 diabetes and may occur before the onset of clinical diabetes. It is more commonly seen in women than in men.
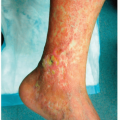
Lesions typically arise as atrophic plaques that are characteristically translucent yellow, red to brown in color as epidermal atrophy and telangiectasias become evident (Fig. 22-2).
As lesions progress, the center becomes depressed and yellowish in color (see also Figs. 18-24 and 18-25)
Ulceration resulting in pain may occur.
 Figure 22-1 Acanthosis nigricans (AN). Axillary AN in the setting of insulin resistance and obesity. The skin has a velvety texture. |
 Figure 22-2 Necrobiosis lipoidica diabeticorum (NLD). Yellow-red, shiny, atrophic patches that appear most often on the shins. |
 Figure 22-3 Diabetic bullous disease. This insulin-dependent diabetic woman has a tense noninflammatory bulla on her dorsal foot. |
The condition is typically chronic with variable progression and scarring.
Diabetic Bullous Disease (Bullosis Diabeticorum)
Diabetic bullous disease (bullosis diabeticorum) manifests as large, tense, subepidermal, noninflammatory blisters.
Lesions most often arise spontaneously on the lower extremities, especially the ankles and feet (Fig. 22-3).
Bullae are asymptomatic unless secondarily infected.
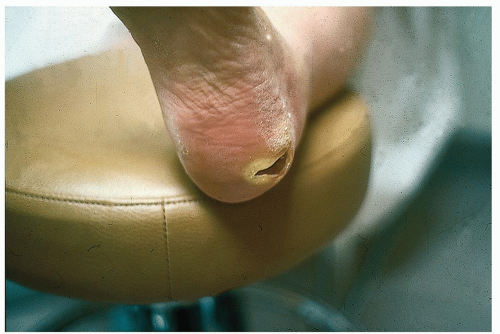 Figure 22-4 Diabetic neuropathic ulcer, mal perforans. This is a nonpainful ulceration at a site of pressure that is associated with a sensory neuropathy. The lack of pain sensation predisposes people to developing ulcers because they lack the normal protective sensation of pain that results in avoiding friction and trauma on the skin. |
Diabetic Neuropathic Ulcer (Mal Perforans)
Associated with diabetic sensory neuropathy, diabetic neuropathic ulcers occur on pressure points such as the heels (Fig. 22-4), great toes, and metatarsal heads.
Painless lesions appear to be “punched out,” often with a hyperkeratotic rim arising in thick, calloused skin.
Thyroid Disease-Associated Lesions
Pretibial Myxedema
Pretibial myxedema is caused by circulating autoimmune γ-globulin, which acts as a thyroid-stimulating hormone. It can appear before, during, or after the thyrotoxic state and it is not related to thyroid function. It is generally seen 12 to 24 months after diagnosis. Found most commonly on the pretibial areas, the dorsum of the feet, or in sites of prior trauma.
Lesions are flesh-colored or erythematous, waxy, infiltrated, translucent plaques (Fig. 22-5; see also Fig. 18-22).
Exophthalmos
Exophthalmos also known as proptosis can affect one or both eyes and is most often caused by thyroid eye disease (Fig. 22-6).
CUTANEOUS MANIFESTATIONS OF LIPID ABNORMALITIES
Abnormalities of lipid metabolism, with high circulating levels of various lipoproteins can result in deposition of cholesterol and other lipids in the skin, tendons, and other organs. Xanthomas consist of the lipids found in tissue macrophages in the skin and tendons. Lipoprotein abnormalities have been classified into primary (genetic) lipoproteinemia and secondary lipoproteinemia resulting from underlying diseases.
 Figure 22-5 Pretibial myxedema, Grave disease. Symmetric, firm, pink, nonpitting dermal pretibial plaques. (Image courtesy of Robert I. Rudolph, MD.) |
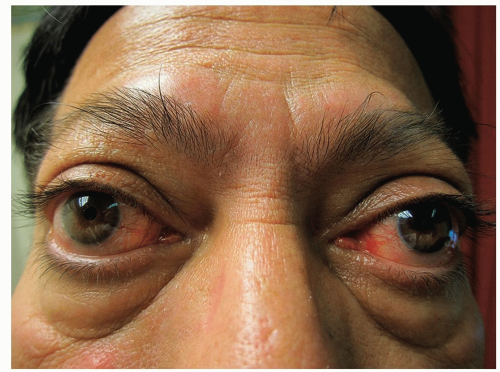 Figure 22-6 Exophthalmos. Eye proptosis, lid retraction, and telangiectasia are characteristics of Grave disease. |
Type IIA, familial hypercholesterolemia: elevated low-density lipoproteins
Type IIB, familial hyperlipidemia: elevated low-density lipoproteins and very-low-density lipoproteins
Type III, familial dysbetalipoproteinemia: elevated intermediate-density lipoproteins
Type IV, endogenous familial hypertriglyceridemia: elevated triglycerides
Type V, familial combined hyperlipidemia: elevated chylomicrons and elevated very-low-density lipoproteins
Secondary hyperlipoproteinemias result from disturbances in cholesterol and triglyceride metabolism caused by cholestatic liver disease, diabetes mellitus, pancreatitis, multiple myeloma, and nephrotic syndrome
Eruptive Xanthomas
Eruptive xanthomas are seen as skin markers for various primary genetic disorders such as certain types of hyperlipidemias or may be secondary to diabetes.
Lesions are smooth, yellow, papular lesions (2 to 5 mm), sometimes with a surrounding red halo.
Eruptive xanthomas arise most frequently over extensor surfaces and pressure points—the knees, elbows, and buttocks (Fig. 22-7).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


