Cryptotia
Akira Yamada
Arun K. Gosain
DEFINITION/ANATOMY
Cryptotia is a relatively rare congenital ear deformity. The upper portion of the auricular cartilage is partially buried beneath the skin on the side of the head, hiding the upper portion of the ear. Cryptotia is often associated with helixantihelix adhesion that results in a narrower helical arc in the upper pole. Cryptotia is also associated with upper helix deficiency that is a manifestation of constricted ear. Cryptotia is more frequent in Asian countries. In Japan, it has been reported in as many as 1 in 500 births.
PATHOGENESIS
The cause of cryptotia is unknown. One theory is that cryptotia is the result of an anomaly of the intrinsic transverse and oblique auricular muscles.1
PATIENT HISTORY AND PHYSICAL FINDINGS
The upper portion of the helix is buried underneath the skin (FIG 1). If one pulls the existing helix, the upper portion of the helix comes out easily. On releasing the helix, the upper helix returns to its initial position buried beneath the temporal skin.
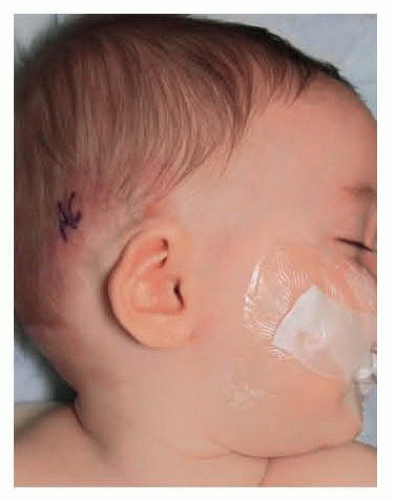 FIG 1 • Preoperative view of cryptotia; the upper pole of the helix is buried underneath the scalp. |
DIFFERENTIAL DIAGNOSIS
Helix-antihelix adhesion
Constricted ear
Microtia
NONOPERATIVE MANAGEMENT
If the patient presents before 1 month of age, nonsurgical correction of the deformity with ear molding techniques may obviate the need for surgery.2
Ear molding techniques are most effective during the first month of life and are unlikely to work after the 2nd month of life.
Helix-antihelix adhesion associated with cryptotia or helix deficiency associated with constricted ear is less likely to resolve with molding techniques.
SURGICAL MANAGEMENT
Preoperative Planning
It is important to check if the cryptotia is associated with other congenital anomalies, such as helix-antihelix adhesion or constricted ear. Pure cryptotia surgery will augment the skin deficiency but will not resolve helix-antihelix adhesion or cartilage defect of the helix associated with constricted ear.
If cryptotia is not associated with cartilage deformities, surgery can be done in early childhood. However, if cryptotia is associated with helix deformities, the authors recommend delaying surgery until at least age 4 to 6 years because of the possible need to harvest rib cartilage.
Positioning
Supine position with both ears prepped, including the temporal hair near the ears
TECHNIQUES
▪ Marking of Z-plasty
Z-plasty flaps are designed along the bandlike contracture above the auricle, while pulling outward away from head (TECH FIG 1A). The length of triangular flap depends on the degree of buried position of helix, but in this particular case, the tip of the triangular flap is located along the hairline margin (TECH FIG 1B,C).
Usually, the length of Z-plasty limb is 1.5 to 2 cm3. The anterior limb of the Z (A-C) is usually placed 5 to 10 mm from the ascending margin of the helix. The posterior limb of Z-plasty (B-D) has a more obtuse angle than does the anterior limb, and the continuous extension of the skin incision is marked beyond the retroauricular sulcus (D-E). If more mobilization of the skin flap is needed, D-E can be extended further down, and a back cut may facilitate movement of the flap toward the skin deficiency behind the upper helix (TECH FIG 2).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








