A combined surgical and orthodontic approach to midface and mandibular distraction optimizes stability and outcomes. Orthodontic considerations include proper planning of the distraction vector, appropriate device use, and thorough follow-up through the consolidation and postoperative period. The dental occlusion must be managed throughout treatment in order to achieve ideal results.
Key points
- •
Dental occlusion is a valuable factor in stability of distraction.
- •
Reliable outcomes can be achieved with good teamwork between the surgeon and orthodontist.
- •
Orthodontic management is critical to the success of craniofacial distraction.
Introduction
Since its advent in 1989, distraction osteogenesis of the craniofacial bones has been a valuable intervention for treating patients requiring extension of the mandible, maxilla, zygomas, or cranial vault. A distraction procedure that transports the maxilla and/or mandible changes the dental occlusion, which can affect patient function and long-term stability of the result. An orthodontist should be involved in distraction procedures from the start of the planning through to the follow-up stages, because dental occlusion is an important factor in the stability of the eventual result and acts as the cornerstone in achieving the final jaw position. Orthodontics can play an essential role during activation, consolidation, and follow-up phases of distraction.
Mandibular distraction
Types of Mandibular Distraction
Tooth borne
Tooth-borne interdental distractors have been used in midface or mandibular procedures, both in the anteroposterior and transverse dimensions. They can be useful in closing large bony defects, both in clefts and after tumor resection. The devices are fitted by cementing stainless steel crowns with an expansion screw between them to the teeth adjacent to the osteotomy site. This technique creates large spaces that are difficult to close orthodontically, and often results in open bites because of poor vertical control and molar extrusion. These devices are useful for increasing alveolar length and volume, but exert forces through the dentition and can cause unwanted dental side effects. It should be noted that their morbidity is significantly less than full jaw distraction (examples of this device can be seen in the Elçin Esenlik and Evellyn M. DeMitchell-Rodriguez’s article, “ Alveolar Distraction ,” in this issue).
Bone borne
Bone-borne devices for mandibular distraction exert forces directly through the osteotomized bone and are fixated on either side of the osteotomy site with the activation screw spanning the bony segments. These devices can be external or internal, and each has its own benefits and drawbacks. The choice of external or internal devices must be considered based on size, shape, and the needs of the patient. External distractors allow movement in 3 planes, are versatile, and are ideal for severely hypoplastic mandibles or for those requiring bone graft reconstruction. However, the device is visible, can cause additional scarring, and is prone to traumatic dislodgement. In contrast, internal or semiburied distractors apply forces directly to the bone, reduce scarring, and are more effective for the vertical vector of movement. They can only distract unidirectionally. Internal devices are fixated by self-tapping screws or pins on either side of the osteotomy and have an arm with an activation screw that extends percutaneously for accessibility. However, they have limited use in severely hypoplastic mandibles.
Hybrid
Hybrid distraction devices are a subset of internal distractors that are anchored to both the teeth and the bone. They can be used in mandibular symphyseal distraction in the transverse plane as well as alveolar distraction in the anteroposterior dimension.
Timing of Distraction
Neonatal
Mandibular distraction can be used in at its earliest stage in neonates. In infants, a severely compromised airway associated with a micrognathia are the usual indications. Mandibular distraction has been used to avoid a tracheostomy or to decannulate patients diagnosed with Pierre Robin sequence. Neonatal and infant mandibular distraction has been shown to be a safe and effective intervention in properly selected patients. However, the developing tooth buds can be damaged, displaced, or destroyed by use of the devices, negatively affecting occlusion in the future. Therefore, families should be appropriately informed when considering this intervention.
Primary/mixed dentition
Distraction of the mandible can be used in patients in primary and mixed dentition with no increase in side effects or complications compared with infants. Note that these patients will continue their current growth pattern, whether it be asymmetric or restricted, and overcorrection should be considered. Tooth buds are more easily visualized at this stage and proper planning of device placement can minimize trauma to the developing teeth.
Permanent dentition
Mandibular distraction of the adult dentition can be performed in response to airway obstruction at the tongue base, severe retrognathia, or trauma. It is planned much the same way, with consideration taken for amount of growth remaining, if any. It may also be planned in conjunction with orthognathic surgical procedures such a genioplasty or Le Fort I for occlusal cants and yaw correction.
Planning Distraction Vectors
The vector of placement is of the utmost importance to ensure movements are executed as expected. In mandibular distraction, the devices are placed in reference to the stable maxillary occlusal plane. The device placement must be stable to avoid deviation to the unstable side or rotation on activation. The planning of these vectors is complex because they relate not only to the position of the mandible but to the occlusal plane as well. For example, planned vertical distraction of the ramus will result in an oblique vector on activation if the device is placed parallel to the posterior border of the ramus rather than exactly perpendicular to the occlusal plane. In contrast, planned horizontal distraction will result in an oblique vector if the device is placed parallel to the inferior border of the mandible rather than exactly parallel to the occlusal plane. In addition, neuromuscular forces alter these vectors on activation and consolidation, which is a reason why continued orthodontic intervention throughout the distraction process is critical to achieving a favorable result. In addition, care must be taken to place paired devices in identical (parallel) positions to avoid creating an asymmetry.
Horizontal
A horizontal vector results in anteroposterior movement and, when a unilateral device is applied, mandibular midline shift to the contralateral side. There are minimal effects on the ramus height, and this is a favorable vector in patients with Pierre Robin sequence.
Vertical
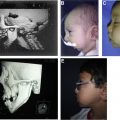
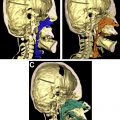
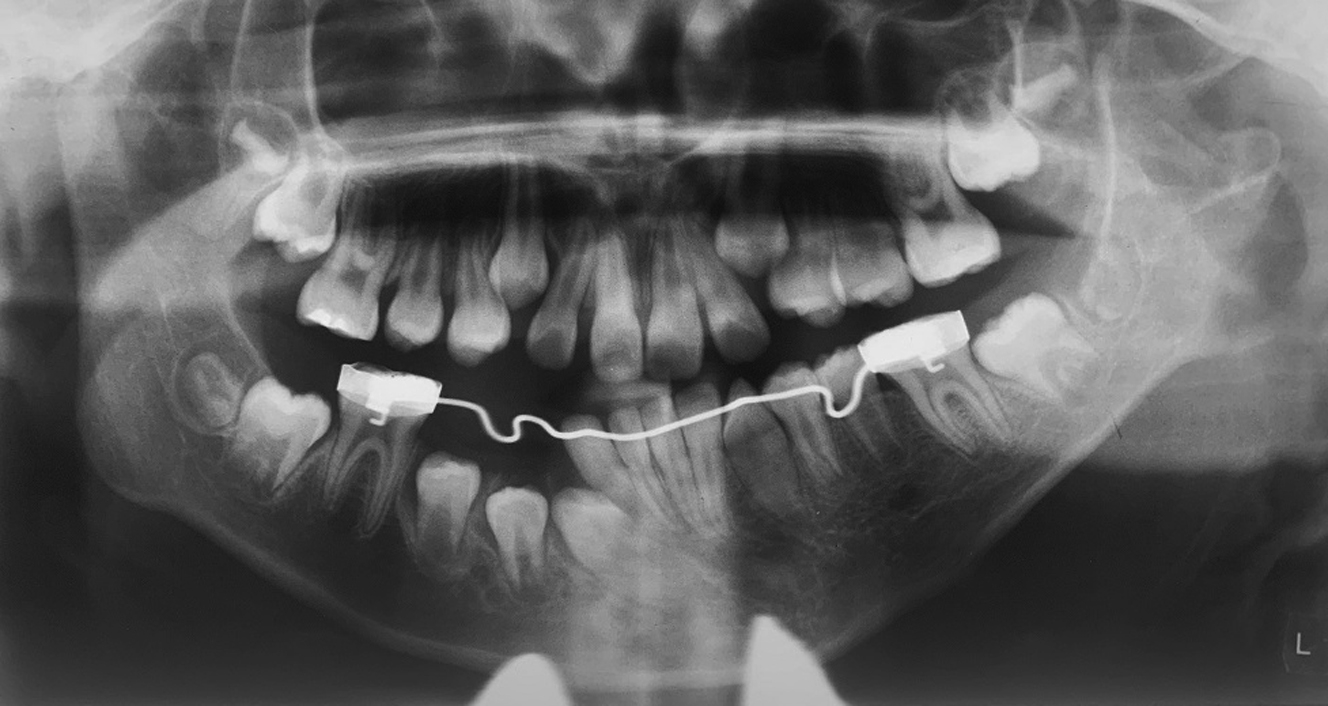
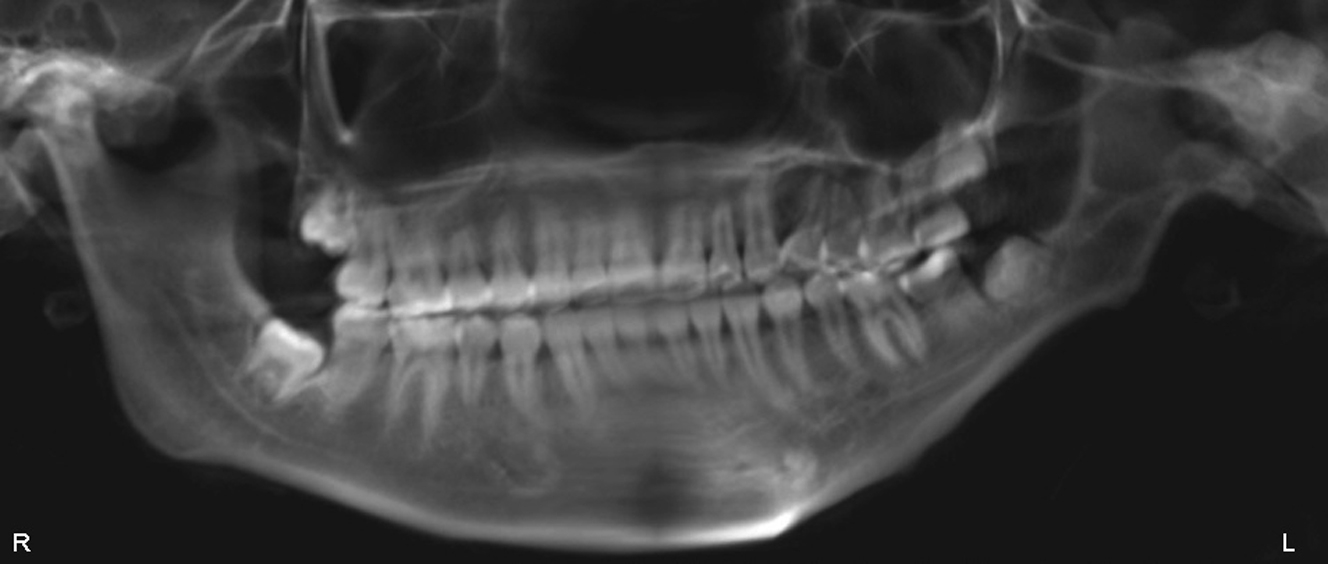
A vertical vector is more useful for counterclockwise rotation of the mandible, causing an increase in ramus height without a marked midline shift. This approach benefits patients with craniofacial microsomia or Treacher Collins syndrome, who tend to have vertically deficient ramus height ( Figs. 1–4 ).
Oblique
An oblique vector can be applied to mandibular distraction to establish a change in both the anteroposterior and vertical planes.
Curvilinear
Curvilinear devices use multidirectional distraction to mimic a more anatomic growth pattern. The devices produce three-dimensional (3D), rotational, and translational movement in the vertical and sagittal planes. Patients with Treacher Collins syndrome can benefit from curvilinear distraction of the mandible, as detailed elsewhere in this issue.
Pretreatment Orthodontics
Planning for the preoperative, intraoperative, and postoperative phases is critical from an orthodontic standpoint to ensure optimal results. Orthodontic evaluation is required preoperatively to assess the skeletal and dental relationships, preparation of the dentition and occlusion, and ideal vector of movement. The assessment is of hard and soft tissues, including position of the lips, corneal exposure, distance from lateral and inferior orbital rims to the globe, occlusal cant, interocclusal relationship, mandibular range of motion, interincisal path of opening, and temporomandibular joint (TMJ) function. Syndromic patients may require ophthalmologic and neurosurgical evaluation before the distraction devices are inserted. All patients must be cleared by a dentist for carious decay and adequate oral hygiene.
Comprehensive records are required for good planning, including two-dimensional/3D photographs, medical-grade computed tomography (CT) or cone-beam CT (CBCT) scan, and dental study models. These records are used to evaluate the craniofacial morphology and idealize placement of the distraction devices. However, soft tissue response and muscle pull are unpredictable by 3D simulation and will have an effect on the final skeletal morphology. CBCT scans can be used for design of cutting and placement guides. If occlusal splints are necessary, these are fabricated using the preoperative records. Orthodontics plays a key role in both planning and execution of the distraction osteogenesis protocol. Orthodontists aim to modify the dentition in relation to the projected skeletal changes, and decompensate the occlusion to fit the final skeletal position.
Maxillary expansion
Orthodontic appliances are often used in order to align the teeth, coordinate the maxillary and mandibular arches, and decompensate the dentition. The narrow maxillary dentition frequently requires expansion to develop sufficient transverse width, because failure to do so will result in an occlusal interference of the dentition during mandibular translation, otherwise known as a functional shift. It is important that the dental relationships aid in good distraction rather than hinder it. Patients often require predistraction expansion of the maxilla to allow sufficient forward movement of the mandible without interference. This approach allows better stabilization of the occlusion through well-coordinated arch forms.
Developing tooth buds
Through 3D surgical planning, orthodontists can idealize device placement to mitigate the negative dental effects of distraction. 3D planning allows visualization of the tooth buds, roots of teeth, and inferior alveolar nerve for proper placement and vector of the distraction device. If extractions are indicated, they should be completed at least 6 months before device placement to avoid damage to the tooth buds or accidental misplacement and to allow sufficient time for bone healing to occur. The tooth buds are not spared in early distraction of the mandible if a mandibular body osteotomy is used. In this case it is usually prudent to extract the second molar tooth buds before treatment. The younger the patient, the more difficult it is to visualize these developing teeth and thus dental injury and future deleterious effects are more likely to occur.
Orthodontics During the Active Phase
Serial radiographs and superimposition
During activation, the skeletal changes must be monitored to ensure the advancement is as planned. There is a latency period of 5 to 7 days that occurs immediately postoperatively, followed by the activation of the distractors. The protocol the authors follow involves a lateral cephalogram taken at the seventh day and every week following until the end of the activation period. Usual activation for mandibular distractors is 0.5 mm twice daily until target mandibular length is achieved. The serial cephalograms are superimposed on one another to track direction and magnitude of movement and ensure fulfillment of the presurgical plan.
Elastics
During activation, orthodontic elastics can be useful to guide the occlusion or individual teeth into ideal position with the newly positioned mandible. They are often used through the consolidation phase to reestablish a stable occlusion and act as a counterbalance to neuromuscular forces.
End point of distraction/planning for growth and relapse
Clinical judgment is required along with analysis of the lateral cephalograms to determine the correct time to stop activation. In order to assess the activation success of a unilateral device mandibular distraction, the notable changes are lowering of the lip commissure, chin deviation to contralateral side, and leveling of occlusal plane. Patients with craniofacial microsomia should be overcorrected beyond the midline to a deviation to the contralateral side to account for the differential rate of growth as the patient ages. When accounting for planned overcorrection, it has been shown that up to 25% of distraction length is lost on average at 1-year follow-up. Therefore, at least 25% overcorrection is required as well as extra accounted for by the remaining growth on the unaffected side. Bilateral devices should be activated equally and monitored for the desired forward or counterclockwise movement of the mandible, depending on the vector of choice. As mentioned, the vector of movement can be affected by muscle pull and soft tissue during activation. It is imperative to monitor for unanticipated vector changes and apply orthodontic elastics as needed to improve direction of distraction.
Orthodontics During the Consolidation Phase
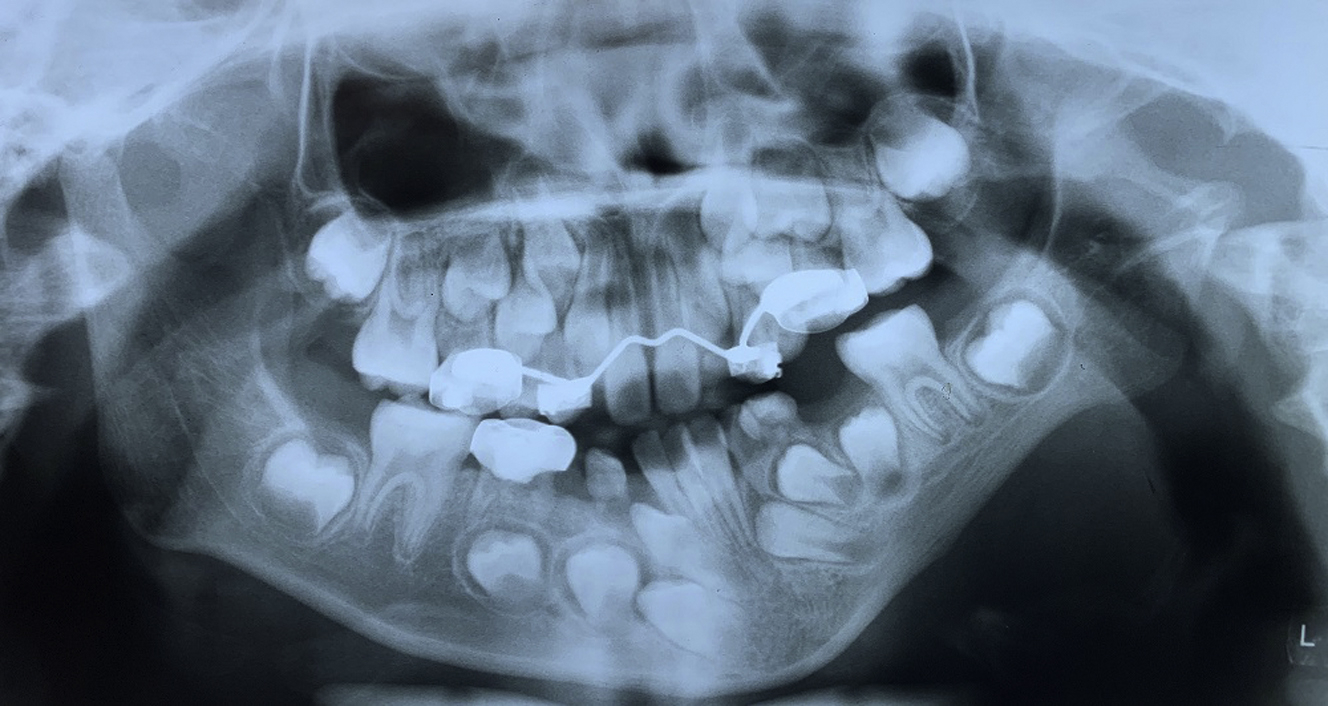
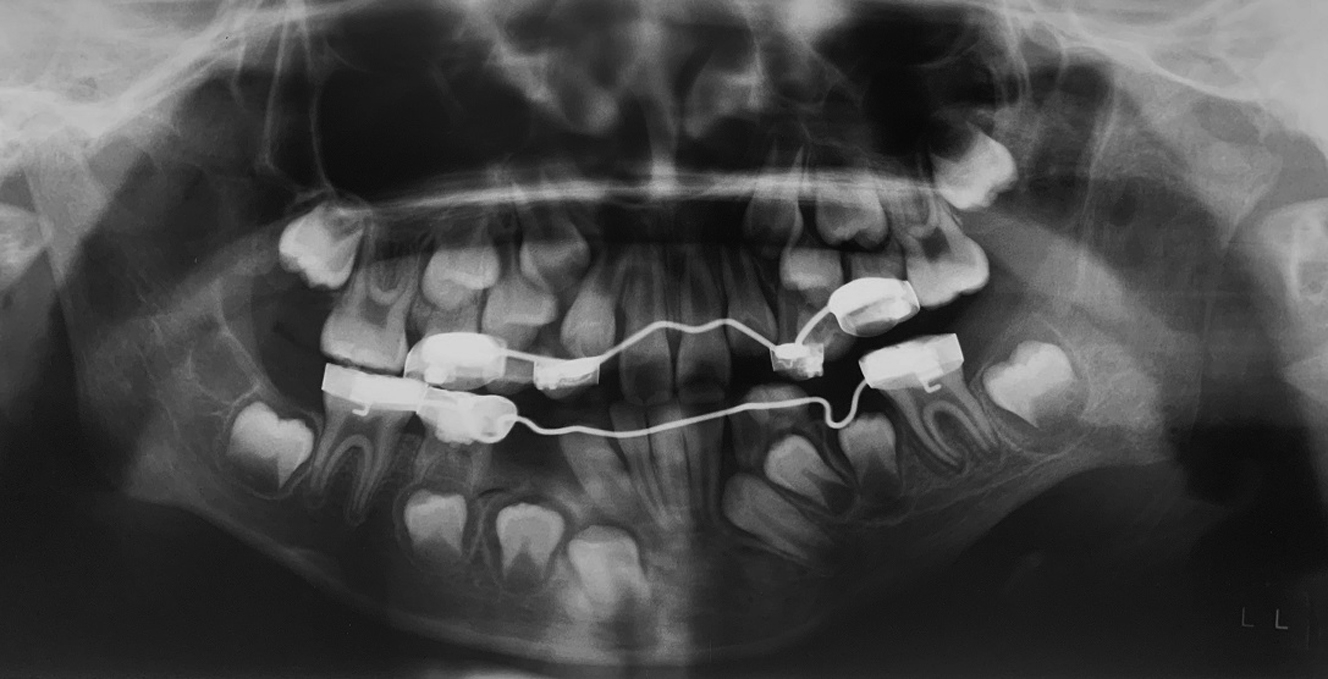
Management of transient malocclusion
There may be interferences unaccounted for or unpredicted movement during activation requiring intervention to mold the generate during the consolidation phase. The consolidation period usually spans 8 weeks after activation is deemed complete. During consolidation and postoperatively, the occlusion must be idealized and the patient should be closely followed by the orthodontist. Often there is significant occlusal adjustment required to establish a stable bite after activation is complete. Note that the actual vector observed often differs from the one planned presurgically, and can be affected by the biomechanics of the individual device, the differences in individual mandibular anatomy, neuromuscular effects, and external force. Fixed braces can be used for patients with adult dentition, whereas bonded splints with hooks may be necessary in patients with short clinical crowns or multiple missing teeth. Temporary anchorage devices (TADs) or intermaxillary fixation screws are useful in all patients for the application of bone-borne forces ( Figs. 5 and 6 ). The forces are ideally distributed over the basilar portion of the jaws to avoid extrusion of individual teeth, and TADs achieve this effectively. Interdental orthodontic elastics used in conjunction with any of the appliances mentioned earlier can assist in molding the bony generate during both the activation and consolidation phases. Heavy elastic forces should be applied immediately during the consolidation phase because they are deemed ineffective at idealizing the alveolus once the bone has consolidated. It is recommended that the distractors remain while elastic forces are being used during the full consolidation period; if removed too early, there can be bending of the bony generate and buckling from the weakness. Interestingly, orthopedic and orthodontic forces are more efficient and effective during these healing phases, likely because of increased bone metabolism after surgical trauma. This finding results in a window of opportunity during which time orthodontic visits should be frequent in order to accomplish treatment goals.