10 Distraction Osteogenesis
Summary
Distraction osteogenesis, the gradual repositioning of osteotomized bone in order to generate new bony matrix, is a powerful tool for transforming the craniofacial skeleton. Compared with conventional surgery, distraction may result in shorter operating times, lesser blood loss, and lesser morbidity, along with simultaneous expansion of the associated skin and soft tissue. This gradual approach may overall engender fewer complications and relapse. However, distraction does require longer overall treatment times and significant familial participation. At present, clinical indications for distraction are expanding, and it represents a major tool in the craniofacial surgery arsenal. A thorough understanding of the current science and the applications of distraction osteogenesis is necessary for any pediatric plastic surgery. Three-dimensional modeling and simulation can provide valuable technological adjuncts in planning and executing distraction treatment plans.
10.1 Introduction
Distraction osteogenesis is a powerful tool in craniomaxillofacial surgery, and its indications continue to broaden. Gradually repositioning the bones of the craniofacial skeleton entails a smaller initial operation and may mitigate the need for permanent rigid fixation. During osseous expansion, not only new bone is generated but also the soft tissue is influenced and adjacent spaces can be enlarged. Smaller devices with improved mechanics and the advent of three-dimensional (3D) analysis and planning have enabled improved patient experiences and outcomes.
10.2 History of Distraction Osteogenesis
Distraction osteogenesis was first described by Codvilla in 1905, where he described using axial distraction forces to lengthen a femur. This was not adopted into mainstream medicine until Ilizarov, a Russian physician, popularized the technique in the lower extremity starting in 1949. The technique was vetted in a series of physiologic experiments, where bone generation was confirmed following gradual traction to the callus. The functional load on bones and their blood supply also showed impact on morphology and articulation points. In parallel, steady traction also encouraged the accommodating expansion of the adjacent soft tissue, including periosteum, blood vessels, ligaments, cartilage, muscles, and overlying skin, known as distraction histogenesis.
In the 1970s, Snyder described lengthening of the canine mandible by using a similar method of bony distraction. This technique was then applied to humans in the early 1990s, to treat patients with Nager’s syndrome and hemifacial microsomia. Since that time, additional craniofacial applications have taken advantage of this powerful tool for gradually lengthening the skull and facial bones, along with the overlying soft tissue.
Throughout the intervening decades, distraction has been used, with significant success in the mandible, and also for alveolar distraction, Le Fort I maxillary advancement, Le Fort II and III midface advancement, monobloc/fronto-orbital advancement (FOA), and cranial vault expansion. As each new technique has evolved, a more thorough understanding of the uses and limitations of distraction has also become more apparent.
10.3 Principles of Distraction
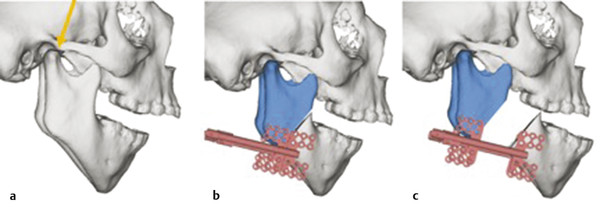
The principle of distraction osteogenesis is straightforward. The procedure begins in the operating room with a carefully planned osteotomy across the region where bony expansion is desired. This osteotomy may be full or partial thickness, depending on the adjacent structures present, and the orientation of these cuts is critical to achieving the desired result. Once the osteotomy is made, a distraction device (internal or external) is applied with grounding footplates or pins on either side of the osteotomy. The vector of this device placement determines the 3D direction of the distraction and bony regenerate formation. Depending on the age of patient, time may be given for a latency period, where the device is held in its original position, with no forces applied across the devices. Once distraction begins, the device is activated and it stretches the span across the osteotomy site. This is done in a slow, controlled fashion, which enables the regenerated bone matrix to form across the osteotomy as it is stretched. Once the desired end position of distraction is reached, the devices are left in place for consolidation. This time period permits the bony regenerate to ossify and strengthen into true new bone. After this, the devices can be removed and the newly generated bone will maintain the distracted length (Fig. 10‑1).
The advantages of distraction osteogenesis include the gradual distraction histogenesis, first described by Ilizarov. Since the two sides of the osteotomy are not extensively manipulated in the operating room, there is less immediate trauma to the tissue, which means less blood loss, less swelling, and shorter operative and hospital admission times. Unlike osteotomies with repositioning and bony fixation immediately in a new location, there is no need for bone grafting, as the bone incrementally forms itself. Distraction may also mitigate future growth restrictions by avoiding need for wide subperiosteal exposure and fixation. With external devices, there is also the opportunity for midcourse vector correction if the tissues do not respond exactly as predicted to the distraction plan. In addition, distraction may be appropriate for smaller children who may not tolerate single-stage bony movement.
Disadvantages of distraction pertain to the hardware requirement and total treatment time. Patients and families are educated that this is not a one-and-done surgery but instead occurs over a period of weeks to months and requires activation and cooperation by the caretakers. The distraction devices, which may remain on for several months, may be distressing to parents if not adequately prepared. Often, much of the distraction is carried out at home, which requires less hospitalization time, but it does require participation of parents to turn the distraction devices and accurately record the protocol. Distraction procedures require a strong treatment relationship and communication between the craniofacial teams and the patients/families under their care, in order to reach a successful outcome.
10.3.1 Scientific Principles of Distraction Osteogenesis
During distraction osteogenesis, a number of critical events are carefully orchestrated at the molecular level. During the distraction phase, bone forms in response to the forces of tension and stress on the regenerate, which heals by membranous ossification. The collagen fibers are oriented parallel to the direction of distraction, and osteoid is deposited in the center of the regenerate. Ossification then advances from either end of the central fibrous zone, which forms an immature bone bridge across the distraction defect. This immature bone then remodels, beginning in the consolidation phase and continuing for 1 to 2 years. Although the regenerate is never as strong as the native bone, it eventually reaches approximately 75% of native bone strength.
Limitations of distraction osteogenesis may occur in patients who have poor local and systemic substrates (Table 10‑1). In addition, devices may become dislodged by trauma or infection, which can result in malunion or nonunion. Longer periods of consolidation may also be cumbersome to some patients. As a result, much recent research has been aimed at increasing bone deposition to possibly shorten the overall treatment time. Rat studies have used adenovirus-driven transcription of the gene for BMP-2 to enhance bony deposition. It is also known that ischemia can be a limiting factor in distraction. Studies have shown that endothelial progenitor stem cells are drawn to this ischemic site during activation and they remain through the consolidation period. These stem cells may represent another possible source to overcome ischemic limitations of distraction. Cyclic mechanical strength has been related to expression of IGF-1, TGF-B, and bFGF along with interleukins (IL)-1 and IL-6, possibly the effectors of further bone growth in distraction osteogenesis. Numerous interventional cytokines have been utilized to optimize bony deposition and possibly decrease overall treatment time. A list of these substances can be found in Box 10.1.
Box 10.1 An Overview of Some Molecular Cytokines’ Interventions and Their Effect on Distraction Osteogenesis
Bone morphogenic protein
Endothelial progenitor cells
Alkaline phosphatase
Transforming growth factor-β1
Vascular endothelial growth factor
Basic fibroblast growth factor (bFGF)
Interleukin 1
Interleukin 6
Local factors | Systemic factors | Distraction factors |
Osteoprogenitor supply Blood supply Infection Soft tissue scarring Bone stock Radiation history | Age Metabolic disorders Vitamin D deficiency Connective tissue disease Steroid therapy Calcium deficiency | Latency period Rate of distraction Rigidity of fixation Consolidation period Regenerate length |
10.3.2 Distraction Protocols
Distraction osteogenesis consists of three general phases: latency, distraction, and consolidation (Table 10‑2). The first stage, latency, occurs after bony osteotomy but before activating the distraction device. During this time, the surgeon allows preliminary callus to form but does not want the regenerate (the intermediate stage of bony deposition) to begin to reossify through calcification. Depending on the bone being distracted, those skeletal components with a richer blood supply or membranous origin (such as the mandible and the skull plates) require shorter latency periods. In addition, younger patients, such as neonates and young infants, may not require any significant latency period before distraction. For mandibular distraction in these patients, the surgeon can either start distracting immediately or wait only 24 hours to begin distraction. In contrast, older patients, who are skeletally more mature, may require a slightly longer latency period, usually 3 to 5 days when distracting the mandible.
Distraction is the phase in which the physical lengthening of the bone is instigated through active manipulation of the distraction device. Using the distraction device, the callus that is formed on either side of the osteotomy site is stretched gradually. During this time, there is exuberant angiogenesis. This vascularized osteoid stimulates new bone formation across the osteotomy defect, which forms parallel to the distraction vector.
Much has been written on the ideal frequency and rate of distraction, and there is significant variation among different authors and practitioners. There must be a balance between distracting too fast, which results in a fibrous nonunion, and distracting too slow, which can cause premature bony union that prevents further lengthening. Perhaps, the most frequently cited rate of distraction is 1 mm/day, generally separated into two daily increments of 0.5 mm. However, distraction rates of 2 mm/day and even 3 mm/day have also been reported. Younger patients, such as neonates, can generally tolerate more rapid distraction, as their bony healing patterns are more robust. The indications of airway creation to avoid a tracheostomy or of cranial expansion to allow brain growth in these patients also generally provoke a more urgent, more rapid course of distraction.
The final phase of distraction osteogenesis is consolidation. During this period, the device is used to maintain the physical lengthening achieved by the distraction period. While the bone is being stabilized in this manner, the bony regenerate can reossify through calcification into a mature bone. The consolidation phase is generally twice as long as the active distraction phase to allow sufficient bone maturation, so that the device is no longer needed for structural stabilization. Consolidation periods of 4 to 12 weeks have been cited, but a period of at least 8 weeks is preferred and has been shown to generally prove sufficient in most cases. Again, younger patients generally require shorter consolidation phases because of their faster healing. Load-bearing bones, such as the mandible, may require longer consolidation periods. When in doubt about an appropriate consolidation period, ultrasound or radiographs can be used to check on the progress of bony remineralization.
10.4 Devices
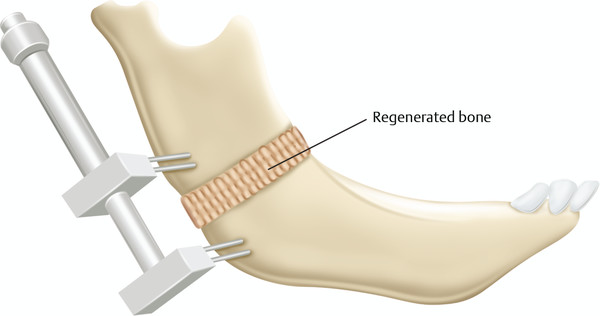
To achieve these goals, a number of different devices have been used throughout the years (Table 10‑3). Initially, external distractor devices utilized transcutaneous pins to fixate either side of the osteotomy site with external distraction arms to exact the lengthening vector (Fig. 10‑2). These devices, with their active parts exposed and available for manipulation, allow for alteration of the distraction vector during the active distraction period. The obvious downsides of these devices include significant bulk and unsightly pin tracks in the skin. Since then, internal devices have been developed. These are placed directly on the bone under the skin and soft tissue; however, periosteum is ideally left intact on at least one side of the osteotomy site to guide the formation of the bony callus. Internal devices also include a distraction arm, which comes through the skin, usually at some length away from the device to discourage infection (Fig. 10‑3). This arm is manipulated to activate distraction of the device. Internal devices can be concealed in a more aesthetic fashion and can be more tolerable to patients and their families, with fewer external components to dislodge. This may permit for longer consolidation periods. However, these can be difficult to securely fixate in very young bone, they must be removed at a second operation, and the vector of internal devices cannot be manipulated during the distraction period.
Device type | Pros | Cons |
Internal | Comfort for patient and family Less obtrusive | Infectious risk Unable to adjust vector Second removal operation |
External | Vector adjustable Single or stage | Cumbersome to patient and family |
Linear | Straightforward Device fixation | Limited dimensions |
Curvilinear | More anatomic | Complex planning Challenging engineering |
Multivector | Precise control Multiple dimensions | Complex planning Require multiple devices Device fixation |

Additional relevant factors include device placement to determine the vector of distraction. In addition to the orientation of placement, devices can be uni- or multidirectional, which will influence the course of distraction based on clinical objectives. Curvilinear devices are also available and implemented in certain contexts (Fig. 10‑4). Many variations of footplates, device arms, and morphologies exist, customized for a wide range of applications.

Resorbable distraction devices have been designed and implemented in patients for many types of distraction osteogenesis. These devices hold the promise of single-stage (or much smaller second stage) distraction protocols that hold the bones in consolidation for a longer period of time but never need to be removed. In addition, programmable, automated devices have been investigated and successfully used in human mandibular distraction osteogenesis in an adult patient. Although these devices have not yet gained widespread use, expandable metal alloys, springs, and pneumatic controls may make distraction protocols simpler for patients and their families in the future.
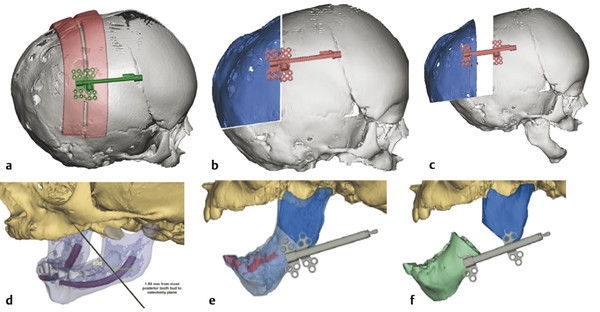
Three-dimensional computed tomographies (CTs) and software planning tools offer improvement to distraction planning and application. An initial CT scan allows a quantitative measurement of the morphology and the existing bone–soft tissue relationships. Computer-assisted design and manufacturing (CAD/CAM) permits virtual surgical osteotomies, device placement, and proposed movements to optimize the clinical result. Three-dimensional prints based on the simulation can then translate the digital plan intraoperatively with cutting guides and templates (Fig. 10‑5). Some have even advocated image-guided and robotically performed osteotomies to further enhance precision in delivering a 3D computer-aided surgical plan.
The distraction plan must incorporate a number of factors. The dysmorphology and deformity must be accurately analyzed, and the goals of correction (size, length, direction, and magnitude) must be accurately defined. Future growth and overcorrection must also be considered. The device type, direction, and placement must be carefully selected and individualized to the patient. The distraction protocol is then discussed with the patient or family at length before beginning distraction, as success is incumbent upon their participation. Consolidation and other retention measures are implemented to maintain the distracted outcome goals with time.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


