5 Orbital Hypertelorism
Summary
Hypertelorism remains a clinical finding associated with a variety of congenital conditions. The severity of hypertelorism can be based on the interdacryon distance and can be used in conjunction with the shape of the frontal-orbital region to better characterize the orbital dysmorphology. The correction of hypertelorism is not a life saving procedure and is mainly an aesthetic procedure when intracranial pressure is normal. Thus, a carefull risk benefit analysis will be required for each case with the treatment plan tailored to each specific deformity and patient related variable. The appropriate choice depends on the relationship between the orbits and the surrounding craniofacial structures:
If the maxillary arch is narrow and the corresponding dentition shows apergnathia with the incisors more cranial than the molars, a bipartition is the operation of choice to improve the maxillary arch and the orbits in the same procedure.
If a unidirectional repositioning is needed in less severe (IOD <35 mm) cases, a box osteotomy is satisfactory. If the orbits are asymmetric with laterally and downwardly oblique positioning, a bipartition is preferred.
Bipartition is the procedure of choice in the most severe cases.
If the nasal structures are narrow, a bipartition and medialization of the upper face can improve the airways by enlargement of the lower face.
An encephalocele associated with a midline cleft can easily be accessed by a bipartition or orbital box procedure. The amount of periobital and midface well can be quite significant. Without tracheostomy, we prefer 72 hours of post surgical intubation and sedation. This allows maximal swelling to occur and begin resolution and ensures adequate hemostasis prior to extubation. Early extubation has led to serious mal-outcomes in our experience and thus our abandonment of this practice. When the patient meets clinical parameters for extubation, it should be performed within 5 days of surgery to assist with patient mobilization and enteral feeding. Blindness, diplopia, and anosmia are uncommon complications, but should be discussed with the patients.
5.1 Introduction
Orbital dystopia can be defined as the abnormal displacement of the orbit and its contents in relation to the adjacent craniofacial skeleton or more specifically in the vertical and/or horizontal planes. Orbital dystopia in the horizontal plane has been termed orbital hypertelorism. Hypertelorism is a symptom or associated finding that can be accompanied by a multitude of craniofacial conditions that are not genetically or epigenetically related. Tessier had classically stressed the fact that hypertelorism is the displacement of the orbital cones in their entirety, manifested by expansion of the central ethmoid sinuses and widening of the sphenoid wing angle to more than 110 degrees. The severity of hypertelorism can be based on the interdacryon distance and can be used in conjunction with the shape of the frontal–orbital region to better characterize the orbital dysmorphology. Patients presenting with orbital hypertelorism will require multidisciplinary specialty evaluation and coordinated care. The specialties include but are not limited to ophthalmology, oculoplastic surgery, psychology, social work, pediatrics, neurosurgery, pediatric dentistry, craniofacial orthodontics, and craniofacial surgery.
5.2 Diagnosis
Orbital hypertelorism is the physical manifestation of excessive and widened ethmoidal sinuses. This orbital anomaly is not pathognomonic of any particular condition but can present in a variety of conditions, including craniofacial clefts, craniofacial dysplasia, and facial craniosynostosis syndromes. Although the term hypertelorism is frequently misused to describe an increased intercanthal distance following trauma or tumors, this process does not cause a change in position of the lateral wall of the orbit or sphenoid wing angle. Hence, most causes of traumatic increase in intercanthal distance are properly termed telecanthus.
The distance between the two medial canthi is known as the intercanthal distance. The distance between the two lateral canthi is known as the outer canthal distance. Interpupillary distance is the space between the two midpupillary points in forward gaze (Fig. 5‑1). All three distances (interpupillary distance, intercanthal distance, and outer canthal distance) are increased in patients with hypertelorism. In patients who suffer from a trauma (naso-orbito-ethmoid fractures), there is usually an increase only in the intercanthal distance, resulting in telecanthus.
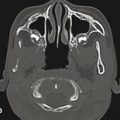
In the preoperative setting, a computed tomographic (CT) scan is recommended as the first-line diagnostic tool. This can detect any previous or ongoing congenital brain malformations. Any malformations identified should be treated by a neurosurgeon in a collaborative and, often, staged reconstructive strategy to optimize outcome. A high-resolution CT scan with thin 1-mm slices will also aid in accurate three-dimensional (3D) reconstruction by limiting the effects of volume averaging of the craniofacial skeleton. In many cases, it can also reveal where certain vital structures are located (e.g., maxillary tooth buds if a Le Fort osteotomy is planned in addition to the orbital repair).
Patients with orbital dystopia may present with a variety of anatomical differences in the anterior cranial base. The ethmoid sinuses, nasal cavity, and sphenoid wings are usually abnormally lengthened. The crista galli and cribriform plates are usually displaced inferiorly, especially in patients with facial clefts. These anatomical abnormalities can cause defects in the anterior cranial base. Appropriate preoperative planning can avoid surgical complications and subcranial strategies such as the Le Fort III osteotomy are the best surgical options. Virtual surgical planning (VSP) has become the de facto standard of care regarding osteotomy design and planning. The cost of VSP has largely been absorbed into the cost of the craniofacial fixation system or distraction system, thus facilitating more widespread adoption. Similar in process to VSP for orthognathic surgery, a more commonly performed procedure, VSP for orbital deformities has added in accurate measurement of the interdacryon distance and thus measurement of the central segment of bone required for optimal correction of the orbits (Fig. 5‑1). We prefer to use an interdacryon distance of 18 mm as the final distance and split the difference equally in symmetric cases or one third to two thirds in asymmetric cases, commonly seen in the X-linked cranial frontal nasal dysplasia syndrome.
It is also important to have the patient evaluated by an orthodontist who is preferably trained for craniofacial deformities. Many craniofacial teams have appropriately trained orthodontists who are comfortable with the management of the difficult occlusion that may present in a patient with hypertelorism as a sequel of his or her craniofacial deformity. Frequently, abnormal position of the orbital cones can directly impact the maxilla. Apertognathia is often seen in these patients, because the smaller ethmoid bones limit the normal caudal rotation of the maxillary ridge in development. In addition, a constricted maxilla with a high arched palate can often be encountered. We prefer the use of the facial bipartition to address the constricted maxillary arch when both orbital constriction and maxillary expansion are needed. In contrast, the orbital box osteotomy is more optimal when only orbital expansion needs correction. Facial advancement and the correction of sleep apnea along with orbital pathology can be accomplished only with the facial bipartition, thus making this operation our preferred and most versatile corrective procedure.
5.2.1 Nonoperative Treatment
The correction of hypertelorism is not a life-saving procedure and is mainly an aesthetic procedure when intracranial pressure is normal. Thus, a careful risk–benefit analysis will be required for each case, with the treatment plan tailored to each specific deformity and patient-related variable. Patients with severe noncorrected congenital heart disease or severe developmental delay who are noncommunicative or vegetative are not considered candidates for surgery because of the unfavorable risk-to-benefit ratio.
5.2.2 Operative Treatment
Corrective surgical procedure for hypertelorism is primarily indicated when the deformity is thought to cause significant facial distortion, resulting in significant poor self-esteem and body image and is in conjunction with a comprehensive approach to the craniofacial skeleton. The upper face and orbits need to be set in their proper position before traditional orthognathic surgery in most patients for optimal restoration of facial balance and harmony. Many patients will have normal mental and physical development despite their often-disfiguring appearances, and this remains a major reason for comprehensive surgical correction of hypertelorism. The goals of surgical corrections of hypertelorism, regardless of cause, should be to:
Normalize the anatomical distance between the orbital cones.
Narrow the nasal width and create an appropriate nasal projection.
Correct any soft diffuse deformities or clefts as well as normalize hair-bearing areas (widow’s peaks or eyebrows).
5.2.3 Operative Timing
All pediatric craniofacial reconstructions are a fine balance between managing appropriate growth of the craniofacial skeleton and optimizing psychosocial development and societal integration. The advantage of operating earlier in life is to address the psychosocial aspects as the developing child becomes more self-aware. The best and most stable results for correction of hypertelorism are obtained after the growth of the cranium and upper one-third of the face or orbits has completed. By the age of 6 years, the majority of the interzygomatic width is established and there is adequate descent of the maxillary tooth buds to facilitate an osteotomy below the infraorbital nerve. Before the age of 5 years, the orbital bones are thin and fragile, which can make the operation more difficult and affect the stability of the fixation, leading to relapse. Most craniofacial centers proceed with hypertelorism correction between the ages of 6 and 8 years. Our preferred age of treatment is 8 years, a time when the upper third of the facial skeleton has completed the growth, but before the development of the frontal sinus, which is typically seen at the age of 10 years.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


