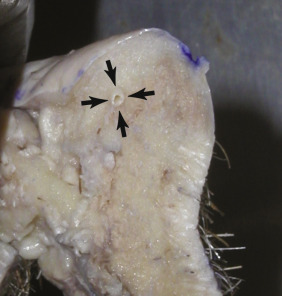
The lips serve many functions: eating, drinking, speaking, mimetic animation, kissing, and serving as a valve for the terminal oral airway. Lips are among the most vascular structures on the face and are supplied by the superior and inferior labial branches of the facial artery as it branches from the external carotid artery. The labial artery lies in the posterior third of the lip at about the incisor level ( Fig. 11.1 ). The depth of this artery is an important landmark to keep in mind, but fortunately, it is deep to most lip-reduction procedures.
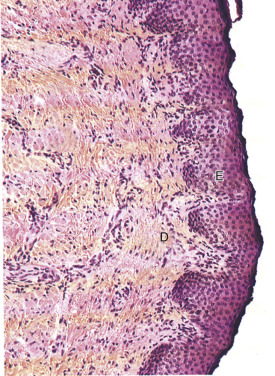
The anatomy of the lip is very unique, in that there is a triple transition from hair-bearing skin to vermilion tissue to oral mucosa. The hair-bearing skin terminates at the cutaneous/vermilion junction. The vermilion tissue consists of a very thin keratinized stratified squamous epithelium with extensive interdigitations with the underlying dermis ( Fig. 11.2 ). The vermilion is devoid of hair follicles, sweat glands, and sebaceous glands (although they may be sparsely present). The lack of sebaceous glands causes the vermilion to dry and crack, and hence the lips must remain moistened with saliva. The vermilion derives its color from the rich vascular plexus in the underlying dermis. This area is also highly sensitive, owing to its rich sensory innervation.
The thin, keratinized stratified squamous epithelium of the exposed vermilion transitions into a thick, non-keratinized stratified squamous epithelium and becomes the intraoral mucosa. Under this thicker epithelium lies a submucosa containing numerous accessory salivary glands, including serous, mucous, and mixed seromucous glands.
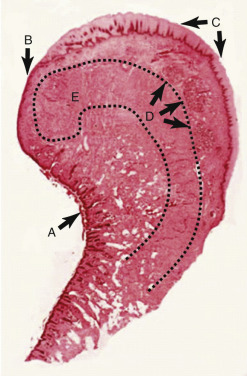
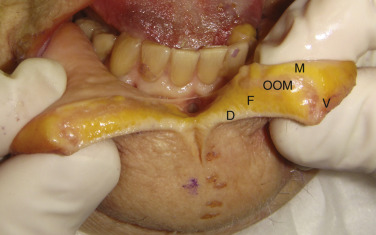
The bulk of the lip volume is made up of the circumoral orbicularis oris muscle, which blends laterally into the complex modiolus, a convergence of the perioral mimetic muscles. The orbicularis muscle lies more to the posterior region of the lip and curls over the vermilion surface and ends at the vermilion/cutaneous junction ( Fig. 11.3 ). Fig. 11.4 shows the lip structures in cross-section.
Surgical Lip Lift
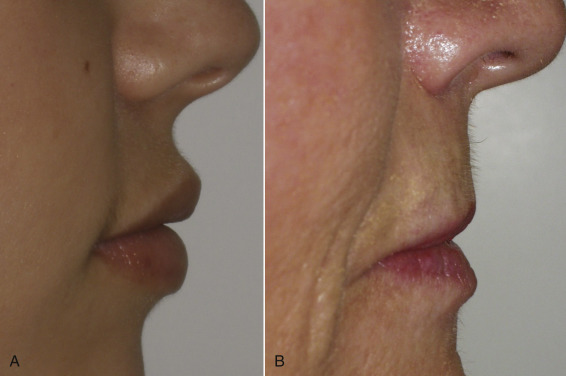
This is also referred to as a subnasal lift, angel wing lift, or bullhorn lift. From time to time, patients come to the cosmetic surgery practice for lip enhancement but anatomically are not great filler candidates. Lengthened upper lips present numerous cosmetic problems. First, the elongated upper lip is unaesthetic; younger patients have short, curvaceous lips with adequate volume. The aging lip becomes elongated, sustains volume loss, and loses its curves ( Fig. 11.5 ). In addition, a long lip can cover the upper teeth and give the patient a “denture” appearance.
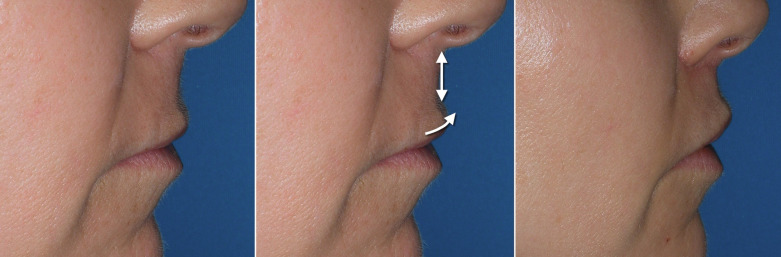
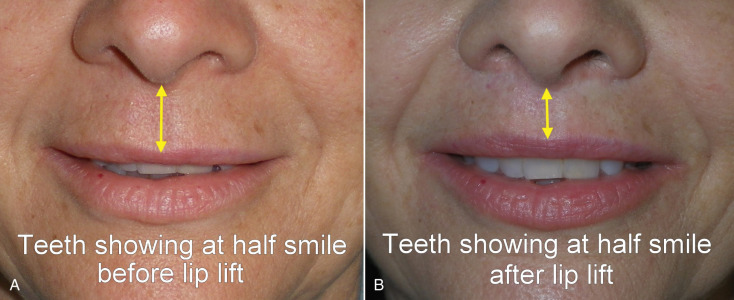
The “lip lift” procedure produces several aesthetic improvements. It shortens the elongated senescent lip to a more youthful, shorter lip and rolls the lip back, which shows vermilion border to provide a more voluminous lip posture ( Fig. 11.6 ). It also allows several millimeters of incisor show, which is considered a pleasing attribute. An attractive smile shows several millimeters of incisor edge exposure in repose and more in smile. Patients that do not show any incisal edge appear older or have an unbalanced smile.
The basis of the subnasal lift is to excise a mustache or bullhorn-shaped piece of skin from the subcolumellar region. When the tissue is excised and the incision closed, the lip is not only shortened (lifted), but the vermilion border is rolled upward and forward. This procedure is only performed on patients with enough vertical lip excess to accommodate reduction without over-shortening. This is important because performing this procedure on a patient with a short lip will expose excessive incisor show and may prevent the patient from being able to put their lips together. The width of the excision is commensurate with the amount of desired lift and can be corrected by 25% to accommodate for relapse. At least 6 mm of skin excision is required for a noticeable result and care is taken to not decrease the lip length to <10–15 mm. This is an arbitrary measurement and many other factors need to be taken into consideration for a balanced appearance. Most cases are performed as a “skin only” excision but some surgeons advocate orbicularis oris excision for severe cases. I have seen numerous cases from other surgeons with dysfunction and appearance problems after muscle excision should be left to surgeons experienced with lip lifting.
Procedure
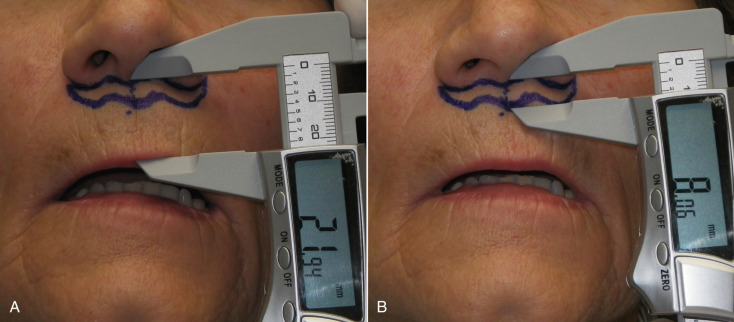
This procedure can easily be performed with local anesthesia, but intravenous (IV) anesthesia may provide a more relaxed patient given that you are operating literally under the patient’s nose. The success of this procedure largely relies on the accuracy of the marking. In this case, it is not only the measurements of the marking but also the delicate curves and tapers. A curvilineal line under the nose is an invitation for a poor aesthetic outcome. The architecture of the alae, columella, and nares require a delicate, curvaceous, tapered incision of the upper extent and a corresponding reciprocal incision on the bottom portion of the incision. Although I have been performing this procedure for almost two decades, I still view a picture of the proposed incision when marking the patient ( Fig. 11.7 ). The incision is marked just inferior to the nasal sill and extends and tapers out from one ala to the other. The incision should not cross the curvature of the nostril sill into the nasal vestibule. The excision is relative to the amount of lip length and generally 6–10 mm of skin is excised ( Fig. 11.8 ).

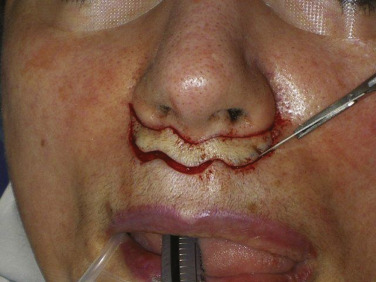
The actual incision is made with a No.11 or No.15C scalpel and it is important to incorporate the delicate outlines of the wings ( Fig. 11.9 ). After the incision is made, I prefer a bloodless modality such as a CO 2 laser or radiowave microneedle to dissect the skin off of the subcutaneous tissue ( Fig. 11.10 ). I do not usually remove orbicularis oris muscle unless it is hypertrophic. After the skin is excised the procedure is basically finished except for the suturing. The peaks and troughs of the incision outline will allow the surgeon to precisely line up the incision edges and this is secured with several subcutaneous 5-0 gut sutures ( Fig. 11.11 ). After the subcutaneous suture a running 6-0 nylon suture is used ( Fig. 11.12 ).

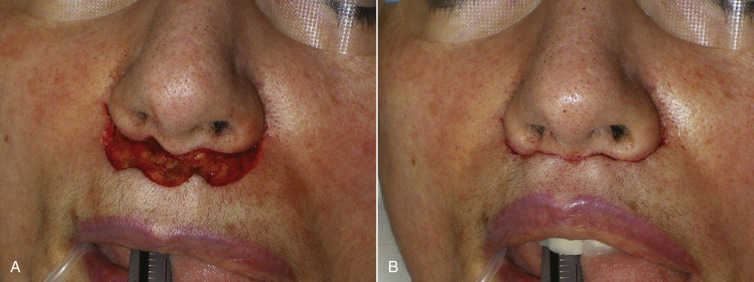

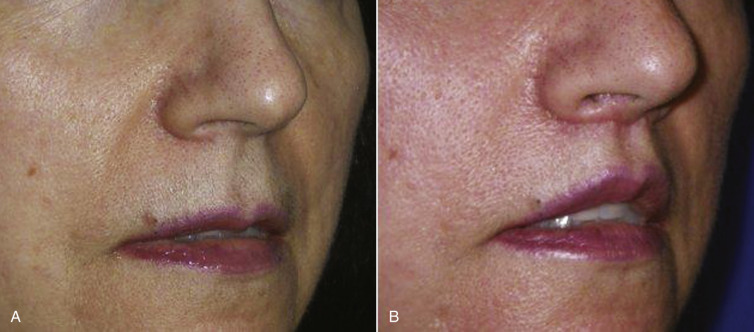
Figs. 11.13–11.18 show selected before and after images for the angel wing lip lift.




Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


