Corneal Neurotization
Joseph Catapano
Ronald Zuker
Asim Ali
Gregory H. Borschel
DEFINITION
Neurotrophic keratopathy is a degenerative corneal disease caused by impairment of corneal innervation.1
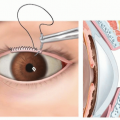
Corneal neurotization involves using functioning sensory nerves from elsewhere on the face as donor nerves to reinnervate the cornea and restore corneal sensation and improve ocular surface health.
ANATOMY
Corneal innervation derives from the ophthalmic branch (V1) of the trigeminal nerve (CN V).3
Lesions may occur anywhere along the course of the corneal innervation pathway including the pons, the trigeminal (gasserian) ganglion, the ophthalmic branch, the nasociliary nerves, and the long ciliary nerves.
Despite corneal nerve density, the cornea is supplied by relatively few trigeminal neurons as a single neuron may support hundreds of individual nerve endings.4,5,6
PATHOGENESIS
Corneal sensation is a necessary component of reflexive tearing and blinking, which prevent corneal injury.
Pain ordinarily would prompt patients to seek appropriate treatment after corneal injuries; however, an insensate cornea leaves patients unaware of their corneal injury.
Corneal nerves also contain neuromediators that promote corneal epithelial maintenance and repair.3,11
NATURAL HISTORY
Neurotrophic keratopathy is one of the most difficult ocular diseases to treat.1
Prognosis is dependent on the severity of corneal hypoesthesia and the presence of other concomitant ocular disorders such as dry eye disease, exposure keratopathy, and corneal limbal stem cell deficiency.
Patients require lifelong treatment and even with optimal management many develop vision loss and blindness in the affected eye.
Inflammation and repeated corneal injury may also result in neovascularization of the cornea, further impeding vision.
PATIENT HISTORY AND FINDINGS
Patients typically present with persistent asymptomatic corneal epithelial defects.
Neurotrophic keratopathy is classified into three stages depending on clinical findings based on the Mackie classification1:
Stage 1: epithelial irregularity with punctate keratopathy and minimal stromal scarring.
Stage 2: epithelial ulceration surrounded by a rim of loose epithelium +/- stromal swelling.
Stage 3: corneal ulceration involving the stroma with risk of corneal perforation.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Diagnosis is based on clinical findings and a patient history of corneal hypoesthesia or anesthesia with delayed healing and persistence of corneal epithelial defects.16,17
Slit lamp: identifies corneal epithelial abnormalities, including diffuse staining with fluorescein, epithelial sloughing, and stromal neovascularization.
Corneal esthesiometry: measures corneal sensation. This can be performed with a Cochet-Bonnet aesthesiometer (Luneau, France) by a skilled ophthalmologist.
Schirmer test: used to diagnose concomitant dry eye disease, when needed.
In vivo corneal confocal microscopy (IVCCM): documents the absence of corneal nerve fibers.
DIFFERENTIAL DIAGNOSIS
Hallmark for diagnosis is the presence of a corneal ulcer and the absence of corneal sensation.
Viral infection (herpes simplex and zoster keratoconjunctivitis)
Chemical burns
Physical injury to the trigeminal innervation (such as intracranial surgery)
Corneal surgery
Diabetes
Leprosy
Topical anesthetic abuse
Congenital (such as trigeminal agenesis, cerebellar hypoplasia, brainstem hypoplasia)
Certain disease may also exacerbate neurotrophic keratopathy:
Dry eye disease
Exposure keratopathy; facial nerve paralysis
Corneal limbal stem cell deficiency
NONOPERATIVE MANAGEMENT
The goals of treatment are to prevent corneal ulceration and promote epithelial healing when ulcerations occur.1,16,17
Preservative-free topical artificial tears
Punctal occlusion
Therapeutic contact lenses (eg, the “Boston lens”)
Topical antimicrobials
Protective tarsorrhaphy
If a corneal perforation is suspected, then cyanoacrylate glue or keratoplasty (cornea transplant) may be indicated.
Exacerbating conditions, such as exposure keratopathy and limbal stem cell deficiency, should be treated.
Experimental treatments for persistent ulcerations include topical IGF-1, substance P, or nerve growth factor (NGF).18,19,20,21Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree