Constricted Ear
Akira Yamada
Julia Corcoran
DEFINITION AND ANATOMY
The concept of constricted ear was proposed by Tanzer.1 The helix and scapha are hooded, and the body and crura of the antihelix are flattened in varying degrees.
Group 1 is the mildest form of constricted ear, often called lop ear, in which only the helix is involved (FIG 1A).
Group 2 is a moderate form of constricted ear that involves helix and scapha.
Group 3 is the most severe form of cupping and is characterized by a tubular structure (FIG 1E).
Differentiation between group 3 constricted ear and microtia can be difficult.
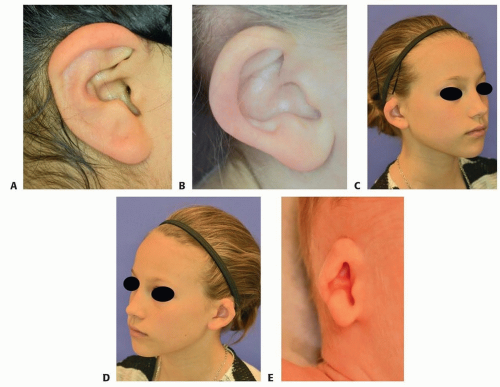 FIG 1 • Tanzer constricted ear classification. A. Group 1: Mild helix cartilage deformity without skin defect. B. Group 2A: Helix and scapha cartilage deformity without skin defect. C,D. Group 2B: Helix and scapha deformities with both cartilage and skin defects. E. Group 3: Most severe form of cupping; characterized by a tubular structure. |
PATIENT HISTORY AND PHYSICAL FINDINGS
Constricted ear is congenital, and the etiology is unknown.
Ear height2 is significantly shorter than normal.
The helix tends to be cupped.
The upper portion of the antitragus (superior and inferior crus) is difficult to see.
The shape of the lower half of the auricle is likely to be normal, especially in mild to moderate constricted ear (see FIG 1C,D).
NONOPERATIVE MANAGEMENT
Nonsurgical manipulation of the ear cartilage in infancy does not work for the constricted ear due to intrinsic deficiency of skin and/or cartilage.
Molding techniques in infancy may change the shape of the auricle but is unlikely to expand skin/cartilage.
“Constricted” means there is cartilage and/or skin deficiencies that must be augmented by surgical procedures.
SURGICAL MANAGEMENT
Preoperative Planning
Age-matched anthropometric data of ear dimension, especially vertical height, help to distinguish deviation of the patient’s ear from norms (FIG 2).
Positioning
Supine position with mild head turn. Both sides should be prepped, even with unilateral surgery, so that the contralateral ear can serve as a normal reference.
Approach
If there is no skin defect and the cartilage defect is mild (Tanzer group 1), the Musgrave4 procedure alone is effective to correct the deformities. If there is moderate skin and cartilage defect (Tanzer group 2B), a local skin/fascia flap plus floating rib cartilage grafting5 is a good choice (presenting case).
If the skin or cartilage defect is severe, microtia surgery6 may be indicated.
Recommended surgical options for skin envelope augmentation, based on the severity:
Mild: Grotting skin flap
Moderate: Park procedure (Grotting skin flap plus fascia flap)
Severe: Nagata microtia construction
Recommended surgical options for cartilage defects, based on the severity:
Mild: Musgrave procedure
Moderate: floating rib (Park)
Severe: total framework (Nagata)
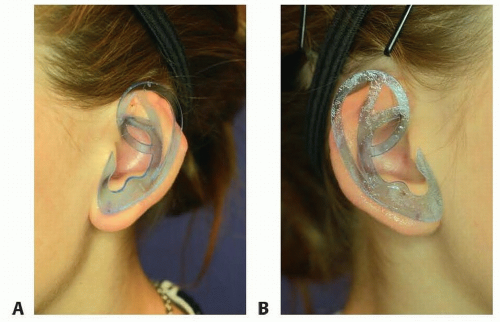 FIG 2 • A type A-2, 48-mm template is used to evaluate the degree of skin and cartilage defect of the upper half of the auricle of the left ear (A) and right ear (B).3 Although the left ear has more severe skin and cartilage defect, both auricles are diagnosed as Tanzer group 2B constricted ear. |
TECHNIQUES
▪ Markings
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


