Abstract
Like all rejuvenative procedures, the aim of facial fat grafting is threefold: achieve a natural appearance by restoring a youthful vibrancy, avoid complications, and attain long-lasting aesthetic benefit. This chapter will attempt to outline a systematic approach toward facial fat enhancement that emphasizes simplicity, consistency, and safety and has been culled through two decades of clinical experience with ongoing technique refinements.
Keywords
Complementary fat grafting, Fat harvesting, Processing fat, Infiltrating fat
History
The history of autologous fat transfer stretches back over an entire century. The first clinical case of fat transfer was described by Neuber in 1893, who reported the use of parcels of fat harvested from the upper extremity to reconstruct a facial defect engendered by tuberculous osteitis . Two years later Czerny commented on filling a breast deformity created by removal of a benign mass with an excised lipoma . In 1910 Lexer described fat transplantation with larger pieces of fat and found that doing so resulted in improved survival . The following year Bruning injected harvested fat into a postrhinoplasty defect successfully and Tuffier used fat placed into the extrapleural space to manage pulmonary conditions . In 1932 Straatsma and Peer used fat to plug fistulas that arose after frontal sinus surgery . Two years later Cotton finely morselized and inserted fat into various defects. In 1956 Peer remarked that walnut-sized fat transplanted fared better than smaller morselized grafts, noting that free fat grafts lose almost half their weight and volume after a year .
The rise of liposuction in 1974 stimulated renewed interest in autologous fat transfer . In 1982, Bircoll reported using liposuctioned fat for contouring a range of defects . In the 1980s Illouz , Krulig , and Newman , based on Pierre Fournier’s work, continued the trend of using aspirated fat for recontouring the face and body. Despite these efforts at autologous fat transfer, the question of viability remained and limited the widespread adoption of this technique. Renewed interest in fat grafting took root as reports of long-term viability began to surface with the use of more gentle harvesting techniques utilizing hand rather than machine suction, and improvements in fat processing with the use of straining and centrifugation . Despite older claims to the contrary, injection of very small parcels of fat appeared to improve survival, as the nourishment of each fat cell is increased by the surrounding neighboring tissue.
Today, proponents of autologous fat transfer have shown the long-term efficacy of fat transfer as well as its importance in facial rejuvenation. Sydney Coleman revolutionized the field of aesthetic facial surgery by putting forth the idea that volume depletion and not gravitational descent represents the primary mechanism of facial aging . He has demonstrated sustained 5- and 10-year facial enhancement results after “lipostructure” fat grafting. Roger Amar has meticulously analyzed the face in terms of the intricate underlying musculature and has based his fat-grafting method on using injections into the respective muscle bellies to achieve aesthetic volume enhancement, calling his unique protocol “fat autograft muscle injection” .
Personal Philosophy
Volume restoration is no longer disputed as a principal mechanism by which the face ages. Autologous fat transfer along with injectable cosmetic fillers have become recognized as important techniques to restore volume in the aging face. Traditional rejuvenative procedures, such as blepharoplasty and facelifts, have been predicated on tissue excision. However, many of these efforts have failed to truly rejuvenate the aging face, resulting in an unnaturally pulled and lifted appearance. Furthermore, traditional procedures may result in an exaggeration or accentuation of age-related volume loss. A new paradigm centered on volume restoration has supplemented rather than eliminated the old paradigm visualizing only gravitational descent of the face and neck. Accordingly, this paradigm suggests that the aging face also suffers from volume depletion over time like a grape that shrinks into a raisin. Therefore, only removal of apparent skin and tissue redundancy can unnaturally transform the face. On the other hand, reinflation of the collapsed face with much-needed volume can restore the face to its natural and youthful form. Autologous fat transfer can play a crucial role in facial rejuvenation as a standalone procedure or in combination with traditional facial rejuvenation procedures ( Fig. 25.1 ) .

Like all rejuvenative procedures, the aim of facial fat grafting is threefold: achieve a natural appearance by restoring a youthful vibrancy, avoid complications, and attain long-lasting aesthetic benefit. This chapter will attempt to outline a systematic approach toward facial fat enhancement that emphasizes simplicity, consistency, and safety, and has been obtained through two decades of clinical experience with ongoing technique refinements.
The use of fat grafting requires the surgeon to acquire a new aesthetic appreciation of the aging process. A new set of skills is required, including fat harvesting and infiltration, as well as management of unique complications. Consequently, we advocate a conservative approach when beginning to incorporate facial fat transfer in one’s practice. In our experience, the postoperative surgical morbidity rate increases as one pushes the limits of fat transfer to obtain ideal results, particularly in the periorbital region. Additional fat transfer in cases of undercorrection is an easier task when compared with the difficulty of managing complications such as visible contour irregularity or an overcorrected face. Conservatism, particularly in the periorbital region, should be the rule, especially for the surgeon inexperienced with facial fat grafting. Since the writing of the first edition of this book, the advent of micro disposable cannulas has allowed for very precise placement of injectable office-based fillers. As a result of these advances, injectable fillers can serve as a simple and more accurate means of volume replacement to touch up a fat-grafting procedure. Accordingly, today it is a far more common practice to perform a primary fat grafting followed by a touch up several months to a year later with injectable fillers to improve the final result when needed.
The new aesthetic principles advocated in volume restoration mandate a different approach to the patient. Rather than arbitrarily defining an aesthetic objective, the surgeon should try to aim at regaining the patient’s youthful appearance. Many surgeons today evaluate a patient during consultation and attempt to define what areas of the face require improvement without reference to how the patient actually looked when younger. For instance, browlifting is usually recommended when the brow appears ptotic. However, a patient may never have had a well-defined upper-eyelid sulcus or arched eyebrow position. Overelevating a brow will often look unnatural and may not return a patient to the way that he or she looked when younger . Volume restoration may be all that is necessary for a patient who always had a low-lying brow that has lost its fullness with age ( Fig. 25.2 ). Patients are encouraged to bring in photographs of themselves when they were younger. These photographs help the surgeon to learn more about the patient’s youthful appearance and the patient to understand the importance of volume loss in the aging process. Reviewing a patient’s old photographs has particular relevance and importance in order to appreciate the role of fat grafting and help the surgeon conceptualize the surgical plan.

Our approach for facial rejuvenation does not rely solely on autologous fat transfer. We have entitled this chapter “Complementary Fat Grafting” to emphasize the complementary role that fat grafting plays in our clinical practices (i.e., a patient’s aesthetic result and satisfaction can be greatly enhanced by using a combination of approaches such as fat grafting, facelifting, blepharoplasty, and even office-based procedures such as neuromodulators, injectable fillers, and laser/light therapies to attain the desired level of improvement). Patients may be considerably more pleased when each procedure adds to the tally of aesthetic improvement ( Fig. 25.3 ). Traditional procedures and fat transfer need not be exclusive of one another. We can embrace two ideologies: autologous fat transfer for volume depletion and lifting procedures for gravitational descent. It is also important, as alluded to, not to forget about the third part of the triad for rejuvenation, that is, the importance of skin treatments such as skin-care products, laser therapy, and neuromodulators. Judicious use of fat grafting with select lifting procedures can constitute a very potent mixture for correcting specific flaws of aging. For example, prominently descended jowls and loose platysmal bands cannot be adequately improved with fat grafting alone. Standard cervicofacial rhytidectomy is often combined with fat grafting of the prejowl sulcus to obtain the ideal aesthetic results. Combining procedures can also diminish perioperative morbidity; fat grafting alone in areas that could be more easily targeted with facelift procedures requires considerable volume, adding to the already long recovery period necessitated by fat grafting. The periorbital region is particularly unforgiving. Selective blepharoplasty to reduce pseudoherniated fat combined with fat grafting along the hollow orbital rim provides the optimal balance of safety and aesthetic benefit. In patients with considerable pseudoherniated fat, the significant volume needed for fat grafting can lead to patient dissatisfaction secondary to increased likelihood for contour irregularity and overcorrection of the region. With ongoing clinical experience, a surgeon will begin to perceive the complementary role that volume enhancement can play in facial rejuvenation.

Although autologous fat has been used successfully to manage hypoplastic lips and depressed facial lines (like the nasolabial and labiomandibular folds), we strongly believe that the rejuvenative benefit for these areas is limited. Fat enhancement of the lips often requires significant fat deposition with marked, prolonged ecchymosis and edema with limited longevity. Similarly, augmentation of the deeper lines in the perioral region often fails to achieve adequate patient satisfaction. We do infiltrate fat into the nasolabial folds when performing fat augmentation of the cheek to ensure that the newly augmented cheek does not exaggerate the apparent depth of the nasolabial folds. Patients whose primary goal is lip augmentation or effacement of facial lines are best treated with one of the many available injectable fillers.
Anatomy
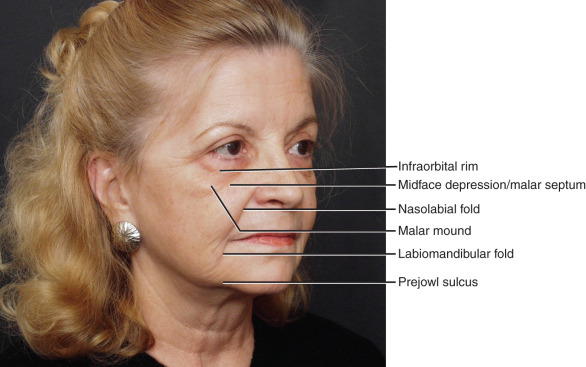
The understanding of facial topography is the most important aspect of anatomy as it relates to fat grafting. The soft-tissue loss that is associated with the aging process is accentuated by the presence of facial retaining ligaments, which create unfavorable depressions ( Fig. 25.4 ). Hills and valleys develop across the surface of the face, contrasting the convexity associated with a youthful appearance.
The face is usually divided into thirds for better anatomic understanding. The upper third comprises the brow and temple area, and the middle third corresponds to the cheek and midface. The lower third constitutes the chin, prejowl, jowl, and lateral mandible. This systematic appraisal will provide a concrete formula for specific volume enhancement based on each individual anatomic territory. Clinically relevant regions of each anatomic zone will be emphasized with pearls to guide surgical strategy.
The Upper Third
The upper third of the face comprises three main constituent elements: the brow, upper eyelid, and temple. A youthful face displays a unified upper-lid–brow complex, much the same way the youthful lower lid flows into the cheek. A younger appearing upper eyelid will have a uniform fullness, from medial to lateral, spanning from the lid fold inferiorly to the brow superiorly; lacking an immediate and pronounced infrabrow shadow typical of an older eyelid . A younger face will also demonstrate a fuller temple, devoid of the shadows at the temporal line and superior border of the zygoma that develop with facial aging. Volume restoration is crucial in minimizing the harsh and aging shadows of senescence that manifest in the upper face.
Important to the analysis of the upper face is an understanding of the varied upper eyelid appearance and the manner in which this affects both the aging process and the techniques for rejuvenation. To simplify, youthful upper eyelids can be broken down into two subtypes. The more common, type I, is characterized by a fuller upper lid with a minimal strip of visible pretarsal skin between the lid fold and lash line. The less common, type II, demonstrates a higher lid fold with a greater degree of visible pretarsal skin, creating a more sculpted superior orbital rim . Regardless of subtype, youthful eyes are characterized by soft-tissue volume camouflaging the superior orbital rim, creating a softer appearance from the presence of an infrabrow highlight ( Fig. 25.5 ).

Advancing age manifests with volume loss of the orbit, particularly in the superomedial aspect, due to bone remodeling as well as fat loss . The medial upper lid has a ligamentous attachment to the orbital rim; as a result, superomedial bone resorption causes a corresponding cephalic retraction on the medial upper-lid fold, manifesting as an A-frame deformity (see Fig. 25.2 ). The bone and soft-tissue volume loss at the superior orbital rim erodes the platform that supports the brow, resulting in a relative brow descent and crowding of the upper lid. Additionally, an infrabrow shadow will often appear and interrupt the youthful continuum from upper-lid fold to brow. Type I upper lids age with great variability, ranging from primary skin redundancy without significant volume loss to primary volume loss. The treatment strategy needs to be tailored to the age-related changes apparent in the individual being evaluated, balancing the need for skin-removal blepharoplasty with volume-oriented strategies. Aging in type II upper eyelids is dominated by volume loss, with skin redundancy playing a much less significant role.
The Middle Third
The middle third of the face is the most complex subunit and perhaps the most important area for facial rejuvenation with autologous fat grafting. This region encompasses the lower eyelid, the malar and submalar areas. A youthful face is characterized by a confluence of the lower eyelid and cheek regions, which becomes separated into visually distinct regions during the aging process ( Fig. 25.5 ). The orbital rim is more clearly observed with aging due to the orbital fat bulging superiorly and volume recession along the inferior orbital rim. The voluminous lateral cheek mound of youth dissipates to reveal the smaller, flatter contour of the malar bony eminence that lacks any notable soft-tissue coverage. The anterior cheek begins to lose volume, developing a linear depression coursing from the nasojugal groove in a inferolateral direction and corresponding with the underlying malar septum ligamentous attachment . Finally, the buccal region can exhibit marked atrophy and should be reconstituted along with the anterior and lateral malar regions to achieve better confluence and to avoid an exaggeration of buccal hollowing following malar augmentation. As an extension of the midface, the nasolabial fold should be deemed part of midfacial volume enhancement.
Restoring midface volume is an important part of creating a more youthful appearance. Unfortunately, as we have seen an increased acceptance and incorporation of adding volume, there has been a corresponding increase in putting too much emphasis on quantity of volume. In particular, there appears an emphasis on overaugmentation of the anterior cheek and the cheek highlight, resulting in a unnatural appearance, especially when a patient is smiling. As with many techniques, sometimes the pendulum swings too far, and in that case it needs to be reset to achieve the natural results we aim for.
The Lower Third
The lower third of the face is principally focused on the labiomandibular fold, prejowl sulcus, labiomental sulcus, and chin. The chin undergoes volume recession as opposed to the volume gain that can be appreciated in the jowl region. For very early jowling, volume enhancement with autologous fat in the prejowl sulcus can be sufficient to straighten the jawline. Even markedly conspicuous jowling is often accompanied by proportionate volume contraction along the prejowl region. Accordingly, facelifting to correct significant jowling can still fail to straighten the jawline if prejowl augmentation is not performed. Volume deficiency in the lateral mandible, posterior to the jowl, may be age related or congenitally absent. The addition of volume to the lateral mandible can help diminish the appearance of the jowl and restore the youthful jaw contour.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


