Clinical Scar Research: Quantitative and Qualitative Assessment of Hypertrophic Burn Scars
Paul Diegidio
C. Scott Hultman
KEY POINTS
To familiarize researchers with some of the most common clinical scar assessment methods.
To introduce three of the most frequently used instruments for measuring and tracking changes in scar quality: the Chroma Meter, Ultrasound, and Cutometer.
To discuss the aspects of clinical trial design.
To discuss current gaps in knowledge about scar treatment.
To discuss what the ideal scar assessment tool/study would need to be included in order to address current gaps in knowledge.
When beginning a new clinical trial for burn scars, it behooves the researcher to first determine how they will assess the scar, how to incorporate subjective data (how the patient feels about the scar pre- and posttreatment), in what ways will the scar be objectively measured, and how the study design will integrate the data being collected into meaningful research. Without a predetermined series of before and after measurements, it is impossible to determine what change, beneficial or otherwise, occurred as a result of the intervention. This chapter will cover some of the most frequently used methodologies in current clinical scar research. Upon finishing this chapter, readers should be able to discuss aspects of scar research and understand the instrumentation and methodology seen in the literature. This chapter is aimed at both novice and expert scar “caretakers” who may be interested in more fully understanding the literature or potentially starting research of their own. As detailed below, ongoing research in scar care continues to advance the spectrum of our treatment modalities. However, knowledge gaps about timing of therapy initiation and ideal type, course, and length of therapy (based on scar characteristics, skin type, type of initial injury, age of scar, etc.) continue to persist. Further, most published scar scales are generally lacking in one area or another, and a comprehensive scar assessment scale does not yet exist. The challenge of mastering each individual scar measurement system may seem an arduous task, but we will attempt to give readers an edge in appreciating these topics, to avoid costly pitfalls, such as time-consuming protocol revisions, in the planning and execution of their research. Conceivably, efforts spent learning the basics in this chapter will save time, energy, and money in the long run; perhaps this is best stated or rephrased by Lewis1: “The longest way round is the shortest way home.”
PEARL 28-1
Clinical trial design can seem daunting at first; however, when approached in a stepwise manner and pursued with diligence and patience, it can be extremely rewarding. As food for thought, there is a discussion at the end of the chapter detailing recent advances in clinical treatment, some gaps in research that still need to be addressed, and some pointers on how to set up the “ideal” research study. Begin by identifying key points where collaborators are needed and think about how you would set up a trial like this at your own institution.
Section 1: Clinical Scar Assessment
Currently, there are over a dozen high-quality, validated, and published scar scales. Modifications and revisions to these scales continue to produce additional versions available to researchers. In a review article by Nguyen et al.,2 the authors assessed the Vancouver Scar Scale (VSS), a Modified Vancouver Scar Scale, Seattle Scale, Manchester Scar Scale, Hamilton Scale, Patient and Observer Scar Assessment Scale (POSAS), a Modified Patient and Observer Scar Assessment
Scale, Matching Assessment of Scars and Photographs, Stony Brook Scar Evaluation Scale, University of North Carolina “4P” (UNC-4P) Scar Scale, the Visual Analog Scale, and the Dermatology Life Quality Index (Fig. 28-1). This review provides a helpful comparison of the scales related to different components of these scars, functional impairment, and quality of life. In their evaluation of these scales, the authors proposed what components would constitute a comprehensive scale. However, to date, there is not a single burn scar scale that captures all of these components effectively. Our review, which follows, selects several of the most commonly used scar scales, which can be combined, so that researchers can accurately describe a hypertrophic burn scar, communicate this with their colleagues, and report data that are consistent, accurate, and reliable.
Scale, Matching Assessment of Scars and Photographs, Stony Brook Scar Evaluation Scale, University of North Carolina “4P” (UNC-4P) Scar Scale, the Visual Analog Scale, and the Dermatology Life Quality Index (Fig. 28-1). This review provides a helpful comparison of the scales related to different components of these scars, functional impairment, and quality of life. In their evaluation of these scales, the authors proposed what components would constitute a comprehensive scale. However, to date, there is not a single burn scar scale that captures all of these components effectively. Our review, which follows, selects several of the most commonly used scar scales, which can be combined, so that researchers can accurately describe a hypertrophic burn scar, communicate this with their colleagues, and report data that are consistent, accurate, and reliable.
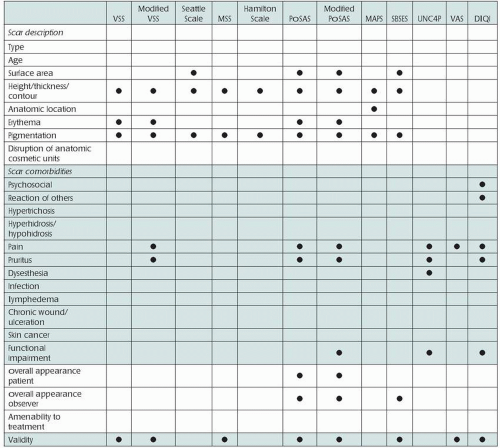 FIGURE 28-1 Comparison of different parameters including currently available scar scales. DLQI, Dermatology Life Quality Index; MAPS, Matching Assessment of Scars and Photographs; MSS, Manchester Scar Scale; PSOAS, Patient and Observer Scar Assessment Scale; SBES, Stony Brook Scar Evaluation Scale; UNC4P, University of North Carolina “4P” Scar Scale; VAS, Visual Analog Scale; VSS, Vancouver Scar Scale. (From Nguyen TA, Feldstein SI, Shumaker PR, et al. A review of scar assessment scales. Semin Cutan Med Surg. 2015;34:28-36.) |
Prior to starting the discussion on each scale and what they measure, it is worth noting that most of the scales in current use combine varying degrees of subjective and objective data. The latter is generally measured by clinicians and includes parameters such as scar height, depth, discoloration, etc., on previously validated scales. There is a small but present subjective component measured by clinicians (i.e., the “overall opinion” section of Observer Scar Assessment Scale), though the vast majority of subjective information is gathered from patients. Most published literature relies on statistically significant changes in objectively measured variables, and the initial study design may focus on finding which scar scale will have the best objective data collected at the end of the study. However, overlooking the subjective portion of outcomes research
would be a grave mistake. Patient care lies at the core of this research, and improving quality of life for individuals who have posttraumatic/postsurgical symptomatic scars is paramount. Pay special attention to the subjective data gathered in the following discussion on scar scales in order to genuinely understand what is being measured and, far more importantly, why.
would be a grave mistake. Patient care lies at the core of this research, and improving quality of life for individuals who have posttraumatic/postsurgical symptomatic scars is paramount. Pay special attention to the subjective data gathered in the following discussion on scar scales in order to genuinely understand what is being measured and, far more importantly, why.
Vancouver Scar Scale
Initially developed in 1990 as the Burn Scar Index by Sullivan et al.,3 this scoring system has become one of the cornerstones of scar evaluation. The VSS measures the scar in four distinct ways and assigns numerical values to the individual characteristics to produce a final score that ranges from 0 to 13:
Pigmentation
Normal = 0
Hypopigmented = 1
Hyperpigmented = 2
Vascularity
Normal = 0
Pink = 1
Red = 2
Purple = 3
Pliability
Normal = 0
Supple = 1
Yielding/gives way to pressure = 2
Firm/inflexible = 3
Banding with rope-like tissues that blanches with extension of the scar = 4
Contracture with permanent shortening of the scar causing deformity and distortion = 5
Height
Normal = 0
<2 mm = 1
to 5 mm = 2
>5 mm = 3
The normal for each category is based on the surrounding unaffected skin or contralateral skin (when available), that is, burned left forearm compared to normal right forearm.
Because of some limitations related to observer bias, the VSS has also been modified to specifically study individual populations.4 For instance, when assessing pediatric burn patients with varying baseline skin color, Forbes-Duchart and colleagues5 modified the Vascularity index to a 6-point scale (normal = 0, pink = 1, pink to red = 2, red = 3, red to purple = 4, purple = 5) and further printed this scale on a clear Plexiglas tool (initially developed by Baryza and Baryza6) to arrive at the resultant 0- to 15-point VSS that they used to evaluate their pediatric burn scar population. This new scoring system was evaluated using inter-rater reliability methodology to ensure ease of use and reproducibility, which should be done with any modification to current scoring systems, as well as validation with current literature.
Patient and Observer Scar Assessment Scale
In 2004 Draaijers et al.7 introduced POSAS as a new, reliable tool for scar evaluation. This scale consists of the Observer Scar Assessment Scale (OSAS) and the Patient Scar Assessment Scale (PSAS), to be completed by the clinician and patient, respectively. Both of these scales use a 1- to 10-point scoring system for each variable, with 1 = normal skin and 10 = worst scar imaginable (with six variables in either PSAS or OSAS; overall scores range from 6 to 60). At the end of either scale, both the observer and the patient are asked to rank their overall opinion of the scar, as it relates to normal skin. The clinician rates six categories, each from 1 to 10, with further descriptors embedded therein that the clinician can select to delineate the specific deformity within each category against comparable normal skin:
Vascularity
Pale
Pink
Red
Purple
Mixed
Pigmentation
Hypopigmented
Hyperpigmented
Mixed
Thickness
Thicker
Thinner
Relief/irregularity
More relief/irregularity
Less relief/irregularity
Mixed
Pliability
Supple
Stiff
Mixed
Surface Area
Expansion
Contraction
Mixed
Overall Opinion
Clinician subjectively rates on a scale of 1 to 10 what their opinion of this scar is.
Patients/subjects are asked to fill out the PSAS, which differs from the OSAS in that it asks subjective questions about how the patient feels about their scar, and rates them as 1 = no/normal and 10 = yes/different than normal:
“Has the scar been painful the past few weeks?”
“Has the scar been itching the past few weeks?”
“Is the scar color different from the color of your normal skin at present?”
“Is the stiffness of the scar different from your normal skin at present?”
“Is the thickness of the scar different from your normal skin at present?”
“Is the scar more irregular than your normal skin at present?”
And finally, “What is your overall opinion of the scar compared to normal skin?”8
Patient-Reported Outcomes Information Management System
Developed by the National Institutes of Health, Patient-Reported Outcomes Information Management System (PROMIS) is “… a system of highly reliable, precise measures of patient-reported health status for physical, mental, and social well-being.”9 With a myriad of available surveys, questionnaires, scales, and rating systems available to physician-scientists, PROMIS serves as a centralized hub to measure patient endpoints using a fully integrated system that is validated and transferrable across disciplines. For example, PROMIS has been used to evaluate patient-reported pain interference, or how pain limits/interferes with an individual’s physical, mental, and social well-being. Amtmann et al.10 published a PROMIS scale developed specifically to evaluate Pain Interference (PROMIS-PI) in 2010. The authors developed a 41-item question bank that provided key information on a given patient’s pain interference, which was then validated and deemed to be a good psychometric test. These questions evaluate pain interference in multiple categories such as concentration, enjoyment of life, participation in leisure activities, day-to-day activities, and family life, to name a few.
The PROMIS-PI differs from previous pain scales in that it allows researchers to evaluate pain from the patient’s perspective of the degree of interference. Traditional 10-point pain scales have been somewhat limiting in differentiating the extent of lifestyle disruption that the patient experiences because of pain or, more to the point, what specifically can be addressed to provide relief from pain or to regain preinjury/presurgical function. Addressing individual issues the patient has with pain interference appears to be a step in the right direction, as previous studies have shown that simply rating the pain on a scale of 1 to 10 does not improve the quality of pain management.11 Although using pain as the “fifth vital sign” brings this important data point to the forefront of medical records, a simple quantitative score—outside of the clinical context—does not add valuable information or assist in clinical decision-making. Additionally, from a research perspective, a validated 41-question scale that can be used to evaluate if the intervention in question provides relief from the burden of pain the patient experiences can be a useful research tool.
Short Form 36/12
The Short Form (SF)-36 is a quality of life survey initially published in 1992, followed 4 years later by an abridged version, the SF-12. This survey tests eight domains in both the full-length and 12-question version: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health. The “role physical” and “role emotional” categories evaluate what physical and emotional limitations the illness has caused the individual. Two versions of the forms exist, either an acute (1-week recall) or a standard (4-week recall) version can be employed. The survey is either administered by a health care professional or self-administered by the patient. After obtaining the data, researchers split the scores into two larger components, the Physical Component Summary (PCS) and the Mental Component Summary (MCS).12 The raw scores are then translated to a 0- to 100-point scale for ubiquity of use and ease of interpretation. The SF-12 PCS and MCS scores correlate well with the SF-36 scores, and the abridged SF-12 has been used in multiple fields since its creation.
As it relates to hypertrophic burn scars, the SF has been used in several studies to evaluate what impact scarring and disfigurement have on the subject’s quality of life. The SF-12 has also been modified to be more specific for a pediatric population, when required. Notably, a study by Kinahan et al.13 in 2012 evaluated the effects of scarring/disfigurement as a result of childhood cancer on long-term survivors’ quality of life. By incorporating SF, the authors were able to better define this population and were able to find statistically significant differences that scarring had on the subject’s emotional distress and quality of life. With any psychometric testing, the larger the body of available preexisting data, the more confidence one can have with these tests. That is, the researcher can be more certain that he or she is measuring what the investigator wants to measure.
Despite a large number of studies that have used the SF-36/SF-12, the literature specific to scars affecting quality of life is somewhat limited. Because of its validated content and ease of use, it is difficult to find a better alternative to measure the quality of life in any scar population, with the exception of burn scars (see below), and the SF-12 is currently employed at the authors’ institution for several ongoing clinical scar assessment studies. With the current and future trials utilizing this instrument, we anticipate that the SF-36, and specifically the SF-12, will become a standard research methodology in the assessment of hypertrophic burn scars.
Burn-Specific Health Scale
Initially published in 1979 by Blades et al.14 in an article entitled “Quality of life after major burns,” the Burn-Specific Health Scale (BSHS) was a 114-item survey used to evaluate the overall health status of burn survivors. The BSHS has undergone several revisions, and currently exists in three forms worthy of discussion. The BSHS-Abbreviated (BSHS-A) consists of four main domains:
Physical—items 1 to 20, subdivided into:
mobility/self-care, hand function, and role activities
Psychological—items 21 to 50, subdivided into:
body image, and affective
Social—items 51 to 65, subdivided into:
family/friends and sexual
General—items 66 to 80, subdivided into:
pain, social sensitivity, and health
The BSHS-Revised (BSHS-R) addressed issues identified by Blalock et al.15 who found that the original BSHS was lacking in the following areas: skin, work, treatment regimens, pain, and itching. The resultant BSHS-R had 41 items covering seven domains of postburn quality of life.
Although the BSHS-R was a much shorter version (and thought to be of more use in the clinical setting), it was followed by the BSHS-Brief (BSHS-B), which was a
40-item, 9-domain scale, scored on a 5-point scale, that combined key elements of the BSHS-R and the BSHS-A. The new domains were Heat Sensitivity, Affect, Hand Function, Treatment Regimens, Work, Sexuality, Interpersonal Relationships, Simple Abilities, and Body Image.16 A year later, a review of the three BSHS (-A, -R, and -B) was performed to evaluate their correlation with each other, and to evaluate which subsets were best covered by these scales. Correlation was the strongest between the BSHS-R and BSHS-B (r = 0.98), followed by BSHS-A and BSHS-B (r = 0.86); the least correlated was BSHS-A and BSHS-R (r = 0.81). The authors also found the smallest respondent burden (i.e., the scale that was the least taxing to subjects) was either the BSHS-B or -R, due to their shorter styles. Additionally, the BSHS-R/-B had a better evaluation of heat sensitivity; and the BSHS-B and -A covered hand and sexual function better than the BSHS-R, bringing the authors to the conclusion that the BSHS-B was the most useful of the three because of both its comprehensive nature and its shorter form.17,18
40-item, 9-domain scale, scored on a 5-point scale, that combined key elements of the BSHS-R and the BSHS-A. The new domains were Heat Sensitivity, Affect, Hand Function, Treatment Regimens, Work, Sexuality, Interpersonal Relationships, Simple Abilities, and Body Image.16 A year later, a review of the three BSHS (-A, -R, and -B) was performed to evaluate their correlation with each other, and to evaluate which subsets were best covered by these scales. Correlation was the strongest between the BSHS-R and BSHS-B (r = 0.98), followed by BSHS-A and BSHS-B (r = 0.86); the least correlated was BSHS-A and BSHS-R (r = 0.81). The authors also found the smallest respondent burden (i.e., the scale that was the least taxing to subjects) was either the BSHS-B or -R, due to their shorter styles. Additionally, the BSHS-R/-B had a better evaluation of heat sensitivity; and the BSHS-B and -A covered hand and sexual function better than the BSHS-R, bringing the authors to the conclusion that the BSHS-B was the most useful of the three because of both its comprehensive nature and its shorter form.17,18
The BSHS-B has yielded promising results since its development and introduction and can be applied to different populations with good internal consistency and validity. It has been used, for instance, in the pediatric population to contrast patients who did and did not suffer from inhalational injury in order to compare their postburn quality of life.19 Although Rosenberg et al.19 did not find that inhalational injury affected postburn quality of life, this publication is a good example of how this shorter, more comprehensive version of the BSHS is an effective tool for evaluating how burn scars may affect study populations.
University of North Carolina 4P
The UNC-4P has been in use at our institution since 2012 as an adjunct to the VSS and POSAS to measure the effect of laser therapy on burn scars.20 The UNC-4P covers the patients’ subjective perception of the scar to include: pruritus, pain, paresthesias, and pliability, which subjects rate on a scale of 0 (best) to 3 (worst), for a combined maximum of 12. In one of our before-after cohort studies, patients reported a mean of 6.0 on this scale prior to the start of laser therapy, and finished the study at a mean of 2.2. Although this scale has not been independently validated, it serves to capture the essence of the patients’ symptoms throughout our treatment phases.
See Table 28-1 for a summary of scales and what they measure.
Table 28-1 Summary of Scales and What They Measure | ||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


