Chapter 21 Classic abdominoplasty with adhesion tension sutures
• The classic abdominoplasty which encompasses excision of excess skin and abdominal wall tightening offers excellent surgical outcomes and patient satisfaction with contour improvements.
• Correct surgical planning and measurements permit an inconspicuous scar that will be hidden in a bikini-style swimsuit.
• The use of adhesion stitches to abolish dead space between the layers has proven effective in reducing the incidence of postoperative seroma.
• Attention to the technical aspects of umbilical inset and contouring will produce a natural-appearing outcome.
Introduction
The history of abdominoplasty starts at the end of the 19th century. Since then new approaches have been introduced continuously by various authors. Its history was published by Hakme,1 Baroudi,2 and Sinder3 in Brazil, and also by other plastic surgeons. This chapter will focus on our experience of five decades in the transverse pubic type of incision. For historical purposes, Monard4 in 1930 was the first to do this type of surgery with umbilicus transposition. Liposuction was used by Illouz5 in abdominoplasty. Pitanguy6 and Bozola7 published their classifications involving both male and female patients. These academic classifications orient the surgeons to select their technique according to the type of esthetic deformity and functional problems. Two patients were selected to illustrate the proposed technique, with different degrees of subcutaneous volume, flaccid skin, and recti diastases. In general the results are different, even performing the same procedures, based on the aspects of the trunk shape, skin quality, the patient’s age, and whether or not liposuction was performed at the same surgical stage, and also by the surgeon’s qualifications. We did not include morbidly obese or post-bariatric patients, but just those with an unesthetic abdominal shape.
Surgical Technique
Three main situations occur in this type of abdominoplasty as described by Baroudi and Ferreira.8
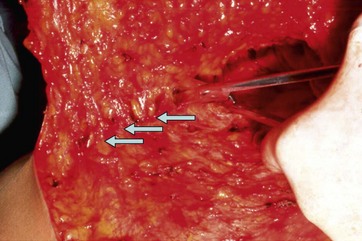
The skin demarcations are shown in Figure 21.1A–D. The surgery starts after previous skin infiltration with saline solution and epinephrine 1: 400 000 in all the demarcated areas. The skin is incised at the pubic level and the incision is extended towards the iliac spines, in general from 35 to 45 cm in length, deep to the superficial fascia level. The skin is undermined at the deep fascia plane up to the umbilical stalk, which is dissected from the skin flap. The dissection concludes near the xiphoid. Above the umbilicus, the dissection narrows to the lateral limits aside the recti muscles in order not to decrease the blood supply to the flap (Fig. 21.2A, B).
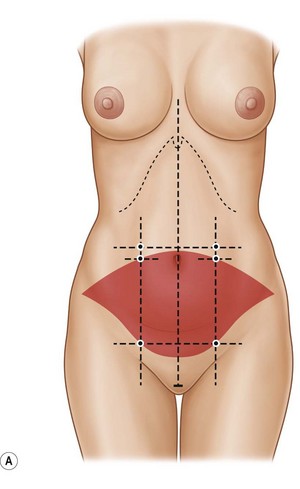
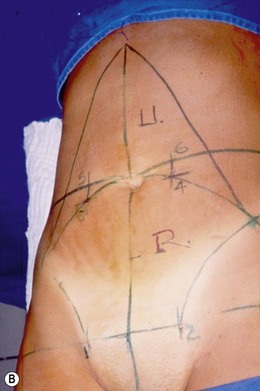

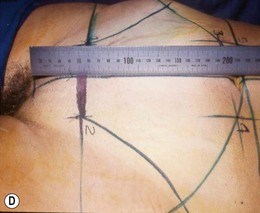

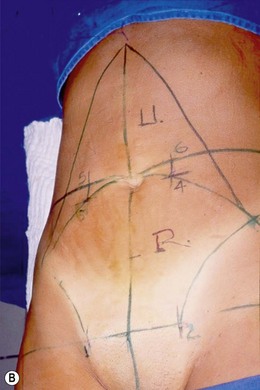
Fig. 21.2 (A) No more extended skin flap undermining, but (B) limited to avoid unnecessary dead space.
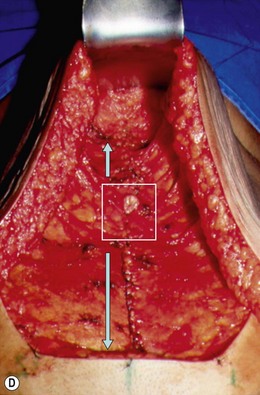
The recti fascia plication is performed in two levels. From the xiphoid to the pubis with isolated nonabsorbable 2-0 stitches with the knot faced downward. Next, a second running suture is applied, also from the xiphoid area to the pubis with a 2-0 nonabsorbable suture. This suture is interrupted 3 cm above the umbilical pedicle and starts again 3 cm below it. Never cross over the umbilical stalk, in order to avoid possible contamination of the nonabsorbable suture (Fig. 21.3A–D).
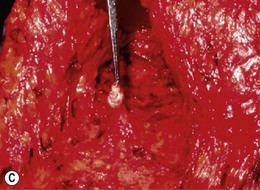
The patient is then positioned with the trunk and the inferior limbs slightly elevated (each at 20°). The undermined skin flap is then stretched caudally; the umbilical hole always surpasses the pubic transverse incision and the excesses are resected. Routinely, several bilateral tunnels are made with scissors along the undermined skin flap limits to release its adhesion and augment its slide caudally, to preserve the flap blood supply (Fig. 21.4). The skin flap is then divided longitudinally in two equal halves and a provisional stitch anchors the flap to the median portion of the pubis. Each skin part is divided again and another two provisional stitches fix the flap to the points (1) and (2) on Fig. 21.4. Finally, all the skin excesses are resected. The provisional stitches are removed and the skin flap elevated with a skin retractor. The adhesion suture (quilting stitch) is applied with absorbable 3-0 stitches in lines and columns from the xiphoid down to the pubis. The distance between them should not be over 4 cm and the amount of stitches should number 40 to 45. From the xiphoid to the umbilical line the skin flap is always stretched slightly after each stitch line is applied.
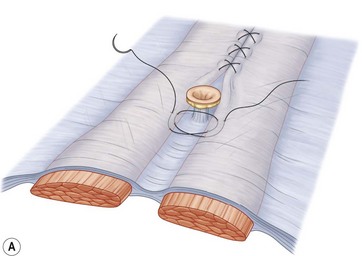
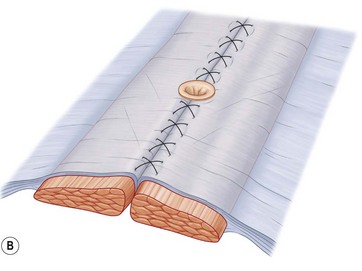
Next, the umbilicoplasty described by Baroudi9 is performed in the following stages:
• Dissection of the stalk, leaving 1 cm of a round skin island at its free extremity. Whatever the pedicle length, two isolated 2-0 nonabsorbable material stitches are inserted at 12 and 6 o’clock, passed through the dermis of the umbilicus and fixed at the fascia level.
• A 2 cm transversal incision transfixes the abdominal skin flap at the level of the umbilicus. Four cardinal position nonabsorbable 2-0 stitches transfix the skin edge flap incision, then the recti fascia below, the skin island, and merge through the open skin flap incision again (Fig. 21.6A–C).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


