8 Choosing the Biopsy Type
A biopsy of the skin is performed to ascertain or confirm the diagnosis of skin lesions, both benign and malignant, and in many cases, to simultaneously remove them. Skin biopsies can be categorized into five types (Figure 8-1):
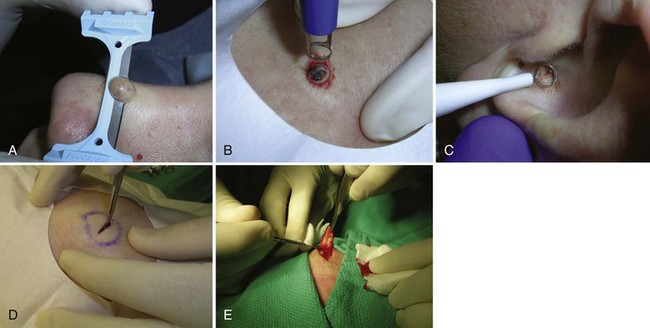
FIGURE 8-1 Five biopsy methods: (A) Shave; (B) punch; (C) curettement; (D) incision; (E) excision.
(Copyright Richard P. Usatine, MD.)
Choosing which type of biopsy to perform influences the diagnostic yield, the cosmetic result, and the cost and time required for the physician to perform the procedure. The clinician must also understand the parameters for selecting that portion of a lesion that will provide the most information to a pathologist.1–3
General Principles
Shave Biopsy
The choice of biopsy technique has much to do with the physician’s initial assessment of the lesion. It is particularly important to consider the depth of involvement within the skin. The shave method is particularly suited to lesions confined to the epidermis and upper dermis, such as seborrheic or actinic keratoses, basal cell carcinomas (BCCs), squamous cell carcinomas (SCCs), and many benign nevi. Chapter 9, The Shave Biopsy, provides detailed information on this topic.
Punch Biopsy
A punch biopsy is the method of choice for most inflammatory or infiltrative diseases and for other lesions in which the predominant pathology lies in the dermis, such as a dermatofibroma. A punch biopsy produces a full-thickness specimen of the skin that, when done properly, extends to the subcutaneous fat. Chapter 10, The Punch Biopsy, provides detailed information on this topic.
Curettement Biopsy
Using a sharp curette is another method of biopsy. A disposable 3-mm curette is a good choice. This size of curette is best suited for difficult areas such as in the canthal folds where the skin is thin and mobile or in areas that are difficult to access such as an ear canal or nostril. Care must be taken not to go too deep and injure vital tissue. A small lesion can be curetted off and sent to pathology (Figure 8-2).

Incisional and Excisional Biopsy
The term incisional biopsy refers to the process of excising a portion of a lesion using full-thickness excision techniques. It is used for obtaining a large sample of a large lesion, but not the entire lesion. The term excisional biopsy refers to full-thickness excision of the entire lesion. Both generally require some type of closure, which is usually done with sutures. See Chapter 11 for more detailed information about elliptical excisions.
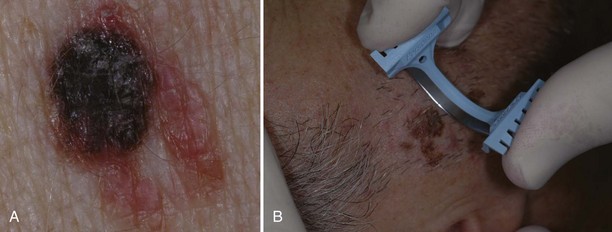
Excision may be the biopsy method of choice for large potentially malignant lesions since a more focal biopsy may miss the malignant portion of the abnormality. Lesions highly suggestive of malignant melanoma (Figure 8-3) are often excised since the resulting specimen will provide a full-depth sample, which is needed for prognosis and treatment. The disadvantages of excising all “suspicious” lesions are that (1) it can lead to overtreatment for benign lesions and more tissue is removed than what is needed, which adds to the cost and increases scarring and other complications (e.g., excising a totally benign nevus or minimally atypical one), and (2) another surgery is often required because the initial ellipse is often performed with margins smaller than recommended for definitive treatment.

The excisional technique is also used to diagnose and remove dermal lesions, subcutaneous cysts and tumors (epidermal cysts and lipomas), and lesions that are too deep or too large to be removed by punch (generally greater than 5 mm in diameter) or shave. Cysts and especially lipomas may be removed with a deep linear incision rather than removing an elliptical portion of the skin (see Chapter 12, Cysts and Lipomas).
Choice of Site to Biopsy
If a “rash” or inflammatory process is present, select a “fresh” lesion that has recently appeared rather than one that has been present longer. Oftentimes, older lesions have been excoriated or secondarily infected, obscuring the primary pathology. Choose a lesion on the upper body rather than the lower body whenever possible (Figure 8-4). The histology may be easier to interpret and the healing should be more rapid. Biopsies of the lower legs are more likely to get infected or have delayed healing. Also avoid the axilla and groin if possible because these areas are more prone to infections.

If a vesicular-bullous reaction is present, it is best to biopsy an intact bulla with some normal tissue (Figure 8-5). It is helpful for the pathologist to examine the edge of the bulla to characterize the exact etiology of the disease process.

FIGURE 8-5 A shave biopsy of an intact blister in a patient with suspected bullous pemphigoid.
(Copyright Richard P. Usatine, MD.)
When direct immunofluorescence (DIF) testing is to be done, biopsies are usually taken from perilesional skin (Figure 8-6). That means the biopsy will not include the bulla or erosion at all. The specimen is generally obtained with a shave or punch biopsy next to the visible pathology. DIF studies are especially helpful for autoimmune bullous diseases because antibodies will light up in the skin (Figure 8-7). They do not have to be done on the initial biopsy but may be performed to clarify and add data to a standard biopsy for hematoxylin and eosin (H&E) staining. There are only a few autoimmune diseases in which lesional skin is preferred (see Table 8-1). A 4-mm punch is adequate. It must be sent to the lab in special Michel’s media (or on saline-soaked gauze). This media should be kept in the refrigerator and can expire. If the cap is on tight and the media has just expired, it is probably still usable. See Table 8-1 for more information on the DIF biopsy.

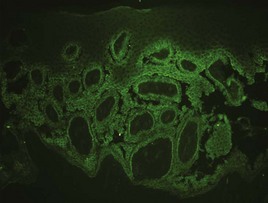
TABLE 8-1 Location for Direct Immunofluorescence Biopsies
Disease | Location of Biopsy | Findings |
|---|---|---|
| Pemphigus vulgaris | Perilesional | Intercellular deposition of IgG. |
| Pemphigus foliaceus | Perilesional | Intercellular deposition of IgG. |
| IgA pemphigus | Perilesional | Intercellular deposition of IgA. |
| Paraneoplastic pemphigus | Perilesional | Intercellular deposition of IgG. Antibodies also directed to simple or transitional epithelium (rat bladder). |
| Bullous pemphigoid | Perilesional | Linear basement membrane staining with IgG and/or C3. Salt split samples will localize to the epidermal side. |
| Cicatricial pemphigoid (MMP) | Perilesional skin, mucosa, or conjunctiva | Linear basement membrane staining with IgG and/or C3. Salt split samples show variable localization. |
| Herpes gestationis | Perilesional | Linear basement membrane staining with C3, IgG is generally less pronounced. |
| Epidermolysis bullosa acquisita | Perilesional | Heavy IgG and/or C3 along the basement membrane zone. Salt split samples will localize to the dermal side. |
| Dermatitis herpetiformis | Lesional or normal skin from disease-prone area | Granular IgA within dermal papillae. |
| Lichen planus | Inflamed, but nonulcerated mucosa or skin | Clumps of cytoid bodies and fibrinogen in the basement membrane zone. |
| Lupus band test | Normal skin | Granular IgG or IgM along the basement membrane zone. |
| Discoid lupus erythematosus | Lesional skin | Granular deposition of IgG, IgM, and/or IgA along the basement membrane zone in conjunction with cytoid bodies. |
| Systemic lupus erythematosus | Lesional skin | Same as for discoid lupus. |
| Bullous lupus erythematosus | Perilesional skin | Heavy IgG and/or C3 along the basement membrane zone. |
| Vasculitis | Early lesion | Perivascular IgA: Henoch Schoenlein purpura. Perivascular IgM/IgG/C3: other forms of vasculitis. |
| Linear IgA dermatitis | Perilesional skin | Linear IgA deposition at the basement membrane zone. |
| Porphyria/pseudoporphyria cutanea tarda | Perilesional | Linear IgG, IgM, and C3 around vessels and dermal-epidermal junction. |
Source: Courtesy of Robert Law, MD.
If a basal cell carcinoma is suspected, it is often easy to shave off the whole lesion. If the lesion is large, almost any area can be biopsied but it is better to select a raised-up border rather than an ulcerated portion. Biopsying the latter may inaccurately provide a pathology specimen that shows only inflammation and reparative debris if not sampled deeply enough. Curettement and punch methods can also be used. An advantage with curettement is that if the tissue is necrotic, it feels “soft” with curetting and also has a classic appearance. The appearance and feel can confirm the initial impression, and treatment can be performed immediately (electrodesiccation and curettage ×3) (see Chapter 14, Electrosurgery).
If a melanoma is suspected, it is best to provide a specimen with adequate depth. Unfortunately choosing the darkest and most raised area does not guarantee the correct diagnosis. Although a full elliptical excision has been considered the gold standard, in some circumstances this is not desirable, for instance, in a large pigmented lesion on the face. In cases of suspected lentigo maligna melanoma on the face, a broad shave provides a better sample than a few punch biopsies and is less deforming that a large full-thickness biopsy. It is also just not practical to perform an elliptical excision on every potentially malignant pigmented lesion. It may be better in some instances to sample the whole lesion with a broad deep shave than to do one or more punch biopsies. Of course, sooner or later, an unsuspecting melanoma may be biopsied with a shave that misses the true depth of the lesion. Note, however, that it is far better to biopsy a lesion—regardless of the method—and find a melanoma early than to delay and procrastinate, thus missing an opportunity for early detection and treatment.4 Suspected early thin melanomas can easily be biopsied with a deep shave technique. When sampling a suspected thick nodular melanoma, a deep sample will be needed to find the Breslow level and plan the definitive surgery. Dermoscopy (see Chapter 32) is a tool that can help you choose the most suspicious area to biopsy in a large lesion if it is impractical to biopsy the whole lesion. Fortunately, nonexcisional biopsies do not negatively influence melanoma patient survival and, in general, do closely correlate with the true depth of the lesion.5,6
Is it cancer?
Pigmented Lesions: Melanoma and Its Differential Diagnoses
Early detection and prompt removal of melanoma can be lifesaving. The early signs of melanoma are summarized as ABCDE, where A = asymmetry, B = borders (irregular), C = color (variegated), D = diameter (greater than 6 mm), and E = evolving and elevation (Figure 8-8).7 Some have suggested adding an F for a change in feeling since some melanomas present with onset of pruritus in a nevus. However, not all melanomas show these signs and not all lesions with these signs are melanomas. The dermatoscope can be used to increase your sensitivity and specificity for detecting melanoma (see Chapter 32, Dermoscopy). Whether or not a dermatoscope is used, it is incumbent on the clinician to biopsy any suspicious pigmented lesion. We cannot overemphasize that patient history is of utmost importance in the evaluation of any lesion and should never be taken lightly. If a patient is concerned that a pigmented lesion has changed, most often it deserves a biopsy/removal.