Introduction
Chemical peels, dating back over centuries, are one of the oldest modalities used for skin resurfacing. With the advent of technology, skin resurfacing saw a spike in dermabrasion followed by laser skin resurfacing and, more recently, fractionated lasers. Interestingly, chemical peels have withstood the test of time and continue to play an important role in cosmetic surgery. If used correctly, they can be tailored to treat almost any skin issue. Furthermore, they can be used to enhance overall results when they are used in combination with laser resurfacing, dermabrasion, and surgical procedures.
Resurfacing implies that the skin surface will be changed. Whether the modality involves laser, abrasion, or a chemical agent, the basic principles of skin type and classification are the same. Regardless of the mechanism of skin injury, careful attention to patient selection and treatment depth is a requisite. Reactive pigmentation disorders, hypopigmentation from overtreatment and post-resurfacing complications can occur with all resurfacing modalities (see Chapter 13 ).
Indications for Chemical Peels
A clear understanding of skin anatomy and the depth of the patient’s pathology is key to selecting the proper level for skin resurfacing. The physician must properly assess the patient to determine what needs to be addressed and the depth of peeling that will be needed to correct this. The most important part of skin resurfacing is to resurface to the proper level, not unnecessarily deeper than needed, nor too superficially.
As the largest organ in the body, the skin has an important role as a barrier to environmental insults, such as ultraviolet radiation, temperature extremes, and environmental pollution. Furthermore, systemic conditions such as hormonal changes, inflammatory skin diseases, and systemic diseases can impact the skin. All together, these internal and external forces give rise to actinic keratoses, solar lentigines, ephelides, dyschromias, rhytids, acne scars, and photodamage, which are among the most common indications for resurfacing ( Table 14.1 ).
| Anatomic skin level | Clinical presentation | Treatment options |
|---|---|---|
| Epidermis | Epidermal melasma | Topical products |
| Actinic keratosis | Superficial peels | |
| Seborrheic keratosis a | Pigment lasers | |
| Solar lentigines (sunspots) | ||
| Ephelides (freckles) | ||
| Dermis | Dermal melasma | Medium-depth resurfacing to deep peels |
| Wrinkles – depth varies | Vascular lasers | |
| Scars – depth varies | ||
| Telangiectasias b | ||
| Sebaceous hyperplasias a | ||
| Syringomas a | ||
| Epidermis and dermis | Mixed-type melasma | Medium-depth resurfacing |
a Best treated with electrodesiccation (using an epilating needle for dermal lesions).
Aging Skin
There are many complex changes that occur as the skin ages (see Chapter 12 ). As skin ages, there is a natural decline in collagen and elastin production and this is known as “intrinsic aging.” However, this decline is accelerated and is more pronounced in environmentally damaged skin, and this is known as “extrinsic aging.” The photoaged skin will also have roughness, dyspigmentation, and keratinocyte atypia in direct correlation to the amount of damage.
Aging Skin
There are many complex changes that occur as the skin ages (see Chapter 12 ). As skin ages, there is a natural decline in collagen and elastin production and this is known as “intrinsic aging.” However, this decline is accelerated and is more pronounced in environmentally damaged skin, and this is known as “extrinsic aging.” The photoaged skin will also have roughness, dyspigmentation, and keratinocyte atypia in direct correlation to the amount of damage.
Patient Evaluation
As with any cosmetic surgery procedures, it is of paramount importance to evaluate and select the patient correctly. Patients seek cosmetic surgery for many reasons, ranging from the obvious to the subtle. Thus, it is very important that the physician presents both what the procedure will achieve and what it will not, keeping the patient’s expectations in check. Showing patients high-quality before and after photographs of a range of treated patients is extremely useful. As with any cosmetic surgery procedure, the most challenging patients, and the ones that require the greatest degree of caution, are those that present with barely noticeable skin defects. These will tend to be the patients that are most likely to closely scrutinize results and to be disappointed in what they may perceive as not significant enough improvement.
Every patient requires a thorough medical, social, and family history to identify possible contraindications to resurfacing ( Table 14.2 ). Certain medications may impact wound healing, such as prednisone or immunosuppressants, while others may indicate an underlying psychiatric disorder. Heavy smokers or patients treated with radiation to the face may have problems with wound healing, as resurfaced skin requires intact and functioning pilosebaceous units and a good blood supply to reepithelialize correctly. Lastly, it is important to enquire about the tendency to develop post-inflammatory hyperpigmentation, hypertrophic or keloid scars, or poor wound healing.
| Pertinent history | Relative contraindications | Absolute contraindications | |
|---|---|---|---|
| Medical | Medications Systemic illnesses Psychiatric illnesses Depression OCD BDD MRSA history Radiation to the treated area HSV or VZV tendency+ | Active acne, rosacea, CTD Vitiligo Bariatric surgery with nutritional deficiency Diabetes Isotretinoin use recently | Active infection at the treatment site History of keloids at the treatment site – avoid reticular dermis-level procedures Pregnancy |
| Social | Smoking history Chronic sun exposure | Smoking/vaping/nicotine use | Inability to follow instructions Unrealistic expectations |
The physical examination should take place in a well-lit room and the patient should have no makeup on. When addressing acne scars, it is useful to have an overhead, movable light fixture to allow the physician to shine indirect light on the skin to highlight certain scars. During the examination, one should also exclude the presence of certain skin disorders that have the propensity to spread to traumatized skin (Koebnerization) (vitiligo, psoriasis, lichen planus, verrucae vulgaris and plana) ( Fig. 14.1 ).

Contraindications to Skin Resurfacing
What gives chemical peels an advantage over other resurfacing procedures is that with the proper skin conditioning as well as the proper procedure depth, patients of most skin types can be treated. However, patients with darker complexions are at risk for permanent hypopigmentation with procedures that reach the depth of the reticular dermis. These are the same patients who are at risk for post-inflammatory hyperpigmentation (PIH) with any procedure. To minimize this risk, the length of preoperative skin conditioning should be extended to 3 months and resumed immediately upon reepithelialization of the skin.
The general health and nutritional status of the patient is also an important consideration for appropriate wound healing, especially in a time where the number of bariatric surgery patients is increasing. Often, post-bariatric surgery patients are deficient in vital nutrients or protein. The physician should enquire about previous poor wound healing, hypertrophic or keloid scars, or a tendency to develop PIH. Seborrheic dermatitis, atopic dermatitis, and rosacea indicate the presence of inflammation in the skin, thus increasing the risk for postoperative complications secondary to alterations in the skin’s normal barrier function. Melasma is a very common dyschromia for which patients seek treatment ( Fig. 14.2 ). However, if the patient is taking estrogen, oral contraceptives, using a hormone-containing intrauterine device (IUD), or is exposed to sun or heat during the recovery phase, she may be prone to a relapse of melasma or a temporary issue with PIH during the healing stages of the procedure.

Concurrent or oral retinoid use within the last 6 months has been generally considered an absolute contraindication to resurfacing due to reports of prolonged healing and hypertrophic scarring. A number of recent studies have brought into question the validity of this concern. These studies of patients on isotretinoin, treated with laser hair removal, laser resurfacing, or medium-depth chemical peels, did not show any adverse outcomes compared with patients not on isotretinoin. This illustrates the complexity of keloid formation. While some of these studies are small, they challenge the conventional thinking that isotretinoin impairs wound healing with regard to skin resurfacing and laser treatments. Until clear-cut guidelines emerge, the author stops isotretinoin 3–4 months prior to resurfacing and does not restart it until 2–3 months postoperatively. If the patient develops an acne or rosacea flare, antiinflammatory antibiotics (doxycycline) can be used for repression without impairing wound healing.
A similar question arises with regards to the safety of simultaneous skin resurfacing and cosmetic surgery. The goal is to optimize results for patients by combining skin resurfacing the same day as their surgical procedure. In the past, it was thought that combining these procedures increased the chance of impaired wound healing. Newer studies have shown safe outcomes when combining fractionated laser resurfacing with short-flap rhytidectomy, full face laser skin ablation combined with rhytidectomy, and fractionated CO 2 laser, browlifting and surgical blepharoplasty ( Fig. 14.3 ).

While most patients can safely undergo skin resurfacing, there are contraindications. The absolute contraindications include pregnancy, active infection at the treatment site, significant tendency to develop keloids, and the inability to adhere to postoperative instructions.
Evaluating Skin Type
When resurfacing skin, the patient needs to be evaluated correctly to help in choosing the correct procedure, depth of treatment, and to help reduce postoperative complications. This evaluation needs to be performed in a standardized fashion. Skin color alone is insufficient in guiding the procedure depth. If one looks more closely, there are some important variations that exist even among patients of the same skin color. Particular attention should be paid to patients that have skin that freckles, develops melasma, or is prone to PIH. Regardless of ethnic background, the presence of these issues heralds the risk of post-procedure hyperpigmentation.
Fitzpatrick phototype is simply a way to type the skin based on the ability to tan in response to ultraviolet (UV) exposure. In this classification, patients are categorized from I to VI as their skin color darkens and their ability to tan rather than burn increases. This classification was intended to help physicians treat patients with phototherapy and is limited, in that it does not address the degree of photodamage present or assist in selecting the correct procedure depth.
Glogau’s classification attempts to objectively quantify the amount of photodamage present but it does not help determine the best resurfacing modality or depth of resurfacing needed. Both of these scales were devised prior to the emergence of nonablative and fractionally ablative technologies and fall short in addressing patients with thicker skin or darker skin types.
The author utilizes the Obagi skin classification ( Table 14.3 ) to help with proper procedure planning. It is a more comprehensive analysis to portend how patients may do in the pre- and post-resurfacing phases and can also be a guide the proper therapy. The Obagi skin classification incorporates five variables that are important to address prior to any resurfacing procedures: skin color, oiliness, thickness, laxity, and fragility. This system helps to identify: which patients require a longer pre- and postoperative skin conditioning program; which patients are more likely to hyper- or hypopigment; which patients are prone to delayed healing; and which patients require a skin-tightening procedure (peels, lasers) over a planing procedure (dermabrasion). The evaluation of all five factors helps to maximize skin-resurfacing results while minimizing complications.
| Skin variable | Skin conditioning – pre- and post-resurfacing | Suitable procedures and potential complications |
|---|---|---|
| Color | Conditioning varies with skin color | Complications related to depth and skin color |
| More aggressive with darker Caucasian skin, and with lighter Asian or lighter African-American skin | Darker skin: | |
| Hypopigmentation: | ||
| Superficial procedure: rare | ||
| Medium-depth procedures: possible | ||
| Deep procedures: more likely | ||
| Hyperpigmentation: | ||
| Common, regardless of depth | ||
| Oiliness | Increased skin surface oil interferes with effectiveness of skin conditioning It may contribute to postoperative acne flares Topical or systemic therapy to control or reduce surface oiliness preoperatively a | Excessive oil hinders chemical peel acid penetration Laser resurfacing is not affected by oiliness |
| Thickness | Thin skin needs papillary-level procedures to thicken the papillary dermal collagen layer Thick skin needs reticular dermis-level procedures to effect a textural change | Thin skin: light- to medium-depth peels Medium–thick skin: good for peels, dermabrasion, fractionated lasers Thick skin: deeper chemical peels, dermabrasion, fractionated lasers |
| Laxity | Lax skin requires long-term collagen stimulation to prevent further laxity | Differentiate between skin and muscle laxity: |
| Skin laxity: medium-depth peel to the level of the papillary dermis | ||
| Muscle laxity: facelift alone or in combination with a medium-depth peel (to correct any associated skin laxity) | ||
| Fragility | Goal is to maintain or possibly increase skin strength | Fragility correlates with post-surgical scarring Procedure depth should be limited to the papillary dermis in fragile skin |
a If systemic isotretinoin is used, it is prudent to delay medium or deep skin resurfacing for at least 3 months (medium-depth resurfacing) to 6 months (deeper resurfacing).
While the concern of permanent hypopigmentation exists, there are some patients at risk for “pseudo-hyperpigmentation.” These tend to be patients with extensive photodamage and they should be approached with caution. “Pseudo-hypopigmentation” refers to an area that once had extensive sun damage and is now resurfaced back to the patient’s baseline skin color and condition. Once the treated area heals, the absence of photodamage may stand out in stark contrast to nearby, untreated, photodamaged skin. This gives the appearance of hypopigmentation of the treated skin. However, when one compares the treated skin to other sun-protected areas, the color of the newly treated skin is not lighter than the patient’s baseline ( Fig. 14.4 ). To minimize this contrast and minimize lines of demarcation, one should consider using topical agents or lighter peels to blend in the skin adjacent to the treated area.

Skin Conditioning
Patients like to see results quickly and instituting a proper skincare regimen can help improve the patient’s appearance while they await their procedure. In fact, for patients on the fence about skin resurfacing, improving their skin with a proper skincare regimen can really motivate them or excite them to move forward with the skin resurfacing procedure.
Improving wound healing is another goal of proper skin conditioning. Patients treated with topical retinoids tend to have a shorter healing time after skin resurfacing. Lastly, instituting an aggressive preconditioning program can help identify patients that may not be compliant with postoperative instructions if they quit their regimen once they develop the initial erythema and desquamation of a retinoid dermatitis. Therefore, the goal of skin preconditioning is to restore the skin, as much as possible, to a normal state prior to wounding it. This is achieved by increasing dermal collagen production, regulating the melanocytes, normalizing keratinocyte atypia, and decreasing surface roughness (to allow more even acid penetration).
Proper skin conditioning should be started at least 6 weeks (8–12 weeks or longer for darker-skinned individuals) prior to resurfacing. Typically, the patient will use this regimen up until the night before the procedure. Tretinoin 0.05–0.1% or retinaldehyde 1% cream promotes collagen synthesis, enhances hydroquinone penetration, restores normal epidermal thickness and maturation, and improves solar elastosis. Studies have shown faster wound healing from skin resurfacing in patients pre-treated with tretinoin. Since many retinoids are photo-labile, it is suggested that they be applied at night. Patients are instructed to apply 0.5–1 g of tretinoin or retinaldehyde to the entire face nightly, including the lower eyelids with feathering to the hairline, jawline, and preauricular areas. The corners of the eyes and mouth should be avoided. The upper eyelids should be treated one to two times per week. If there is significant retinoid dermatitis, the topical agents can be stopped 4–7 days prior to skin resurfacing.
Hydroquinone inhibits tyrosinase, a key enzyme in melanogenesis within the melanocytes. Hydroquinone remains the gold standard in skin lightening to which other lightening agents are compared. Hydroquinone 4% cream is used to suppress melanocyte activity (melasma, lentigines) and to help blend in areas adjacent to the treated areas. Twice-daily application of hydroquinone is required, since it has a half-life of 12 h. Hydroquinone serves another important function. By decreasing the epidermal hyperpigmentation, it will unmask any dermal pigmentation that may be present. If dermal pigmentation is present, then one must choose a resurfacing modality that will reach the pigment. However, as will be discussed later, resurfacing procedures that penetrate into the reticular dermis are at increased risk for complications. Patients are instructed to apply 1 g twice daily to the entire face, with a second light application to areas of darkest pigmentation (sun spots, melasma).
Acne-prone patients, very oily-skinned patients, or those with severe dyschromias will require the use of a daily polyhydroxy acid/lactobionic acid (PHA) or alpha-hydroxy acid (AHA) 6–8%. It helps acne by exfoliating the stratum corneum. The thinning of the stratum corneum also enhances the penetration of tretinoin and hydroquinone. PHA and AHA can deactivate retinoids, therefore their application should be limited to the morning rather than the evening.
Patients must be instructed in the importance of daily sunblock to prevent further dyschromia and sun damage, no matter what skin color they have. In addition to the deleterious effects of UV radiation, there is growing evidence that visible light may play a role in the aging process. Hopefully in the future, we will see an evolution in sun protection to be effective in the visible light spectrum. However, current sunblock protection is mainly for ultraviolet A (UVA) and ultraviolet B (UVB), with some protection in the visible light spectrum if they contain zinc oxide or titanium dioxide. Zinc oxide and titanium dioxide are physical sunblocks and are usually well tolerated by patients. Furthermore, it is important to avoid sun exposure or tanning the skin for 6–8 weeks before surgery, since it stimulates melanin production.
The use of proper skin conditioning prior to a procedure cannot be emphasized enough. In addition to helping reduce the risk of hyperpigmentation post-resurfacing, the pre-resurfacing use of skincare products helps improve skin texture, thus motivating patients to proceed with further procedures to enhance their skin ( Fig. 14.5 ). The ability of a patient to adhere to a skincare regimen helps to predict which patients are most likely to be compliant with postoperative instructions.

Post-resurfacing skincare is restarted immediately once the wound is reepithelialized and the patient is able to tolerate the application of topical medications. Since reepithelialization time varies with wound depth, it may be as early as 3 days (with exfoliative procedures) to as late as 14 days. Post-inflammatory hyperpigmentation may not be clinically evident until 3–4 weeks after the procedure but it starts to form once the wound has healed. Since there may be a delay until it shows up, it is easier to try to prevent it by treating the skin prophylactically, rather than to deal with this frustrating issue once it has occurred.
All resurfacing can be performed as light, medium, and deep in terms of treatment, recovery, and depth. All surgeons must be able to differentiate what treatment depth will benefit given conditions. Modern skin scanners or simple ultraviolet light can be of great assistance, especially to the novice doctor. Epidermal melanin enhances with UV light and patients with dark enhancing pigmentation indicates more superficial melanin deposition (see Fig. 13.9 ). Pigmentation that does not enhance with UV light may be dermal and very resistant to treatment. Performing UV skin evaluation is helpful to educate the patient on their degree of damage, the expected effect of resurfacing, and also serve to show improvement after treatment.
Herpes Prophylaxis
Prior infection with herpes simplex virus (HSV) or varicella zoster virus (VZV) can result in a situation where the virus lies dormant for many years or decades until some form of trauma triggers a reactivation. Reactivation of these viruses can lead to devastating consequences as a result of disseminated cutaneous infection. Since all skin-resurfacing techniques have the potential to trigger virus activation and replication, treatment is aimed at the prevention of outbreaks. It is the author’s preference to treat all patients with valacyclovir (Valtrex; Glaxo Smith Kline, Research Triangle Park, NC) 500 mg by mouth twice a day for 7 days (medium-depth peels) to 14 days (deeper peels or laser resurfacing) until the skin has fully healed. This regimen is started 1 day prior to the procedure for all patients. However, if a patient has a history of frequent HSV outbreaks, the author increases the dose of valacyclovir to 1 g, twice a day, starting 1 week prior to the procedure and for 7–14 days afterwards. The use of antibiotics or anti- Candida agents is best used only if an infection develops rather than empirically on every patient. However, the author does prescribe topical mupirocin ointment to be applied to the nares three times a day, starting 1 week before their skin resurfacing and to continue until their skin is fully healed. This has greatly reduced an already low incidence of impetigo.
Chemical Peel Skin Resurfacing
This chapter describes peels based on their depth of penetration into the skin. Wounds confined to the epidermis (basal layer and above) are called here exfoliative or light peels. Medium-depth peels refers to peels that are a papillary dermis-level peel. Deep peels extend into the reticular dermis. The depth of peels is monitored by intraoperative signs, as discussed below.
Mechanisms of Actions
Often, one will hear peels referred to as “light” or “deep” depending on the type or acid used, or the concentration of the acid. This is misleading and can be dangerous, since there are many factors that affect peel depth, not just concentration or the type of acid. Acid concentration, the number of coats applied, skin thickness, percentage body surface area, skin preconditioning, and in some cases, the duration of contact of the acid on the skin, are the main variables. The trained physician knows to look at the peeling agents based on their mechanism of action, either keratolytic agents or protein denaturants, rather than the concentration that is being used ( Table 14.4 ). The keratolytics are mainly used for superficial, exfoliative procedures, whereas the protein denaturants can be used for superficial or deeper peels.
| Acid properties | Commonly used concentrations and formulations | |
|---|---|---|
| Keratolytics | Salicylic acid peels 15–30% | |
| Glycolic acid 50–70% | ||
| Jessner’s solution | ||
| Phenol 25–50% a | ||
| Protein denaturants | Trichloroacetic acid 15–100% | |
| Phenol 60–88% | ||
| Baker–Gordon phenol peel: | 50% phenol, 2.1% croton oil | |
| Hetter phenol peels: | 50% phenol, 0.7% croton oil | |
| Hetter “all around”: | 35% phenol, 0.4% croton oil | |
| Hetter VL (neck and eyelid): | 30% phenol, 0.1% croton oil | |
| Stone V-K: | 62% phenol, 0.16% croton oil | |
| Stone 2: | 60% phenol, 0.2% croton oil | |
a Phenol at concentrations below 50% has keratolytic properties.
Keratolytics
Keratolytics are acids that disrupt the adhesions between the keratinocytes thus causing shedding of these layers. The two main acids used for exfoliative procedures are glycolic and salicylic acid. However, there are peels based on lactic acid, mandelic acid, citric acid, resorcinol, retinoic acid, and a variety of combination peels that combine more than one agent (i.e., Jessner’s solution). Jessner’s solution is comprised of 14% each of resorcinol, salicylic acid, and lactic acid, mixed in ethanol.
Salicylic acid and Jessner’s solution have an advantage over glycolic acid, in that salicylic acid is lipophilic. Therefore, these two peel solutions penetrate acne lesions or oily skin better than a hydrophilic agent such as glycolic acid. Another advantage they have over glycolic acid is that salicylic acid and Jessner’s solution do not require the skin contact time to be closely monitored.
The main role of keratolytic peels is to address superficial conditions such as roughness, acne, and mild dyspigmentation. These are often referred to as “lunch-time” peels, as these exfoliative acids have the benefit of little to no “downtime” for the patient, no anesthesia requirement, and are easy to perform. Clinical results take time and repeated treatments to become apparent. The results of these peels can be enhanced greatly by the addition of a good skincare regimen that the patient follows at home.
Protein Denaturants
Trichloroacetic Acid Peels
Trichloroacetic acid (TCA) remains the mainstay of medium-depth peeling agents and has a proven safety record. TCA works by causing protein coagulation and denaturation as it penetrates the skin. It coagulates proteins that make up the cells of the epidermis and dermis, as well as the blood vessels. Once it penetrates the skin, it cannot be neutralized. Instead, it self-neutralizes once it is has coagulated a certain amount of protein. Therefore, a subsequent application will continue to drive the peel deeper until it is used up by coagulating proteins deeper down in the skin. When used correctly, it can be used to achieve a variety of peel depths, ranging from exfoliation to deep peels. Of utmost importance when using TCA is to make sure that the acid is purchased from a reliable source that uses the weight to volume (W : V) method to calculate concentration. There are four methods to calculate concentration, but the W : V method is by far the safest. The author uses a 30% TCA solution, which is then modified as part of the Blue Peel, to create a 15%, 20%, 22%, or 25% solution.
It is incorrect to refer to TCA peels as light or deep according to TCA concentration. As mentioned before, acid concentration is just one of the variables affecting peel depth. For example, 1 mL of 40% TCA applied to the face will result in penetration to the basal layer while 6 mL of 40% TCA applied over the same body surface area will result in penetration to the mid-dermis or deeper. Higher volumes will drive the peel even deeper.
With proper training, the physician can tailor peels to penetrate to certain depths just as one would dial-up laser settings. These variations in peels have risen up giving the physician more control over the peel. These are the modified TCA peels (Jessner–TCA peel, glycolic acid–TCA peel, the Blue Peel). These peels are designed to peel to a depth of the papillary dermis and into the most superficial aspect of the reticular dermis. Their main indications are for epidermal and upper dermal pathology: photodamage, actinic keratoses, lentigines, ephelides, fine rhytids, and very superficial, non-fibrotic scars. These peels will not address deeper scars or rhytids.
These combination TCA peels can be categorized as being “accelerated” or “decelerated.” In an attempt to speed the penetration and depth of TCA peels, two modified peels were created, which incorporate the use of a keratolytic agent. The Jessner–TCA peel utilizes Jessner’s solution (keratolytic), applied prior to the application of TCA. Application of the Jessner’s solution allows for faster and deeper penetration of the subsequently applied 35% TCA. A similar mechanism is employed with the glycolic acid–TCA peel, which uses 70% glycolic acid (keratolytic) prior to application of 35% TCA.
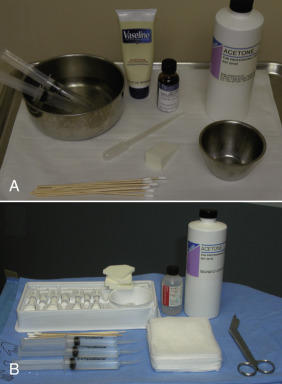
The Blue Peel is unique in that, instead of increasing the speed and depth of the peel, the process is slowed down. This allows the physician better control of depth during the peel. The Blue Peel incorporates a non-ionic blue dye, glycerin, and a saponin with a specific volume of 30% TCA to yield a 15%, 20%, or higher percentage of TCA–Blue Peel solution ( Fig. e14.1 ![]() ). Use of TCA, a colorless solution, requires close attention to avoid reapplication over previously treated areas. Therefore, the blue dye is advantageous, as it stains the stratum corneum and helps the physician to visualize even application of the peel. Since TCA is hydrophilic, the use of a saponin as an emulsifying agent creates a homogenous TCA–oil–water emulsion that penetrates the skin in a slower and more even fashion. TCA peels ( Fig. 14.6 ) can be performed with the Blue Peel mixture or with TCA as the sole agent.
). Use of TCA, a colorless solution, requires close attention to avoid reapplication over previously treated areas. Therefore, the blue dye is advantageous, as it stains the stratum corneum and helps the physician to visualize even application of the peel. Since TCA is hydrophilic, the use of a saponin as an emulsifying agent creates a homogenous TCA–oil–water emulsion that penetrates the skin in a slower and more even fashion. TCA peels ( Fig. 14.6 ) can be performed with the Blue Peel mixture or with TCA as the sole agent.