The face and/or scalp is involved in almost all affected infants
Skin lesions present with varying amounts of ill-defined, scaly, erythematous, edematous, papules and plaques on the cheeks, forehead, and scalp
Lesions are bilaterally symmetric with classic red, glazed, scaly cheeks (Fig. 7-1)
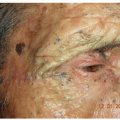
Oozing and secondary infection (impetiginization) with Staphylococcus aureus is common. Impetiginization of eczema is characterized by yellow or varnish-colored crusting overlying the eczema lesions (Fig. 7-2)
Sleep is disturbed due to associated pruritus
The infant is often irritable and itchy as indicated by rubbing the scalp and head on crib bedding, by pinching, scratching, or tapping the skin
Clinical
Eczematous lesions are often present elsewhere on the body
Atopic predisposition such as asthma, seasonal allergies, chronic rhinitis, or atopic dermatitis in the patient’s family
 Figure 7-1 Infantile atopic dermatitis. Acute red, glazed, scaly eczematous plaques on the cheeks and chin of an infant. |
 Figure 7-2 Infantile atopic dermatitis, impetiginized. This infant’s cheek is infected (impetiginized) with S. aureus. |
Despite popular belief to the contrary, patients with AD, especially children, should be bathed daily
The benefits of bathing include removal of excess dirt, potential irritants, allergens, and surface microbes. Bathing also hydrates the skin and allows for better delivery of topical corticosteroids and moisturizers
Baths should be short—no longer than 10 minutes—with tepid water. “Bleach baths” can be helpful in cases of recurrent infection. This is done by adding 1/4 to 1/2 cup of Clorox Bleach to a full adult bathtub
Use of mild, moisturizing soaps such as Dove or Baby Dove or nonsoap cleansers such as Cetaphil
Pat dry followed immediately by the application of a topical corticosteroid to areas of active dermatitis
Suggested ointments: Vaseline Petroleum Jelly, Aquaphor
Suggested creams: CeraVe cream, Cetaphil cream
Topical steroids: A low-potency topical corticosteroid (TCS) such as 1% hydrocortisone cream or ointment (Cortaid) is often recommended to begin therapy; however, using such a low-potency agent may prove to afford little relief and may eventually prolong therapy, especially if the eruption is severe. Therefore, short-term use of a mid-strength TCS such as hydrocortisone butyrate 0.1% (Locoid cream) to a higher-strength TCS such as triamcinolone 0.1% (Kenalog) or even clobetasol 0.05% ointment can be used to initiate therapy for a day or two (“strong, but not long”).
Nonsteroidal immunomodulators: tacrolimus (Protopic ointment) 0.03% or 0.1 % ointments and pimecrolimus cream (Elidel) may be alternated with topical steroids.
Alternatively, crisaborole 2% ointment (Eucrisa), a phosphodiesterase-4 inhibitor, is also a nonsteroidal agent. It is approved for the treatment of eczema in children >3 months of age. If the child’s skin is very inflamed, crisaborole may sting.
The childhood phase of AD follows the infantile phase beginning at around 2 years of age and continues through puberty. Lesions, which often continue to involve the face, also begin to localize to the flexural aspects of the elbows and knees (antecubital and popliteal fossae), the wrists, ankles, and the posterior neck in a symmetric distribution. Lesions may also occur on the lips, scalp, and behind the ears.

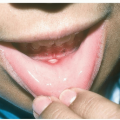
Figure 7-3 Kaposi varicelliform eruption (eczema herpeticum).
Multiple intact and hemorrhagic vesicles, as well as hemorrhagic crusts are evident in this 14-year-old boy. Lesions resolved with minimal scarring after oral antiviral treatment.
Itchy, scaly, erythematous plaques appear on the face
Frequently become infected (impetiginized) with S. aureus
The secretion of toxins (superantigens) by S. aureus may trigger relapses of AD; also herpes simplex virus may attack the relatively defenseless eczematous skin and result in Kaposi varicelliform eruption (eczema herpeticum) (Fig. 7-3) which requires treatment with oral or systemic antiviral medications, such as acyclovir or valcyclovir
Similar to that of the infantile phase described above
There are few areas of the skin that are ignored by eczema. The predominant areas of involvement continue to be the flexural surfaces (see Figs. 13-9, 13-10, 13-11); in addition, the dorsal aspect of the hands and feet are also commonly affected. Lesions also may appear in other extensor locations such as the shins, ankles, feet, and the nape of the neck. Sometimes lesions are limited to the lips (atopic cheilitis), eyelids, vulvar or scrotal areas
For mild-to-moderate involvement, topical steroids and nonsteroidal immunomodulators (as described above) may be adequate to control disease
For moderate-to-severe disease that is recalcitrant to topical therapy, dupilumab (Dupixent), a targeted biologic therapy that inhibits signaling of interleukin-4 and interleukin-13, key proteins that may play a role in the inflammation underlying atopic dermatitis, is FDA approved for patients over the age of 6 years. Dupilumab is administered by subcutaneous injection. Dupixent is effective and side effects have been mostly minimal; an important side effect that must be discussed with patients is conjunctivitis
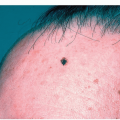
A PWS presents at birth as a flat, well-demarcated, pink to dark red (“port-wine” color) blanchable patch, most commonly noted on the face (Fig. 7-4)
PWSs are usually unilateral but can be bilateral

Figure 7-4 Port wine stain (nevus flammeus).
Port-wine stain in the typical location on the face. Note the sharp midline demarcation. (Image courtesy of Robert I. Rudolph, MD.)
Lesions darken progressively and can become thickened over time. Some develop secondary proliferative nodules on their surface
The diagnosis is made clinically. Workup for an underlying association such as Sturge-Weber syndrome is based on the location of the PWS, especially when a child is born with a facial cutaneous vascular malformation covering a portion of the upper or the lower eyelids
A complete physical examination should be performed to assess for any other congenital defects. If a PWS in a high-risk location is identified, an appropriate workup and referrals should be made
Once a potential syndrome association has been ruled out, the PWS can be approached as a cosmetic issue and treated (especially facial PWS) with various lasers, if desired
 Figure 7-5 Infantile hemangioma. Infantile hemangioma on the eyelid. Had this lesion not been treated, it might eventually interfere with this child’s visual development. (Image courtesy of Robert I. Rudolph, MD.) |
An early IH (macular phase) may be difficult to distinguish from a port wine stain
Asymptomatic or slightly itchy
Present as one or more round, oval, or irregular whitish patches or thin plaques, with or without fine surface scale
Often appears following sun exposure because tanning of surrounding skin unmasks affected areas
Clinical, atopic dermatitis may be noted elsewhere on the body
 Figure 7-6 Pityriasis alba. Ill-defined hypopigmented slightly scaly patches on the cheeks are characteristic of pityriasis alba. |
No treatment is necessary, but a moisturizing cream may improve the dry appearance
If the patches are red or itchy, a low-potency topical steroid cream such as hydrocortisone 1% can be applied
KP presents as an eruption of grouped, follicular, tiny keratotic papules resulting in a sandpaper-like texture when palpated
Distributed in a grid-like pattern
In children, the lateral sides of the cheeks are frequently involved (Fig. 7-7)
Usually worsens during the winter months

Figure 7-7 Keratosis pilaris.
Small, follicular, rough-textured, hyperkeratotic, papules are present on this 2-year-old’s cheeks. Note similarity to infantile acne in Fig. 7-10.

Figure 7-8 Keratosis pilaris rubra faciei, inflamed.
Multiple hyperkeratotic follicular papules overlying facial erythema. (Image courtesy of Robert I. Rudolph, MD.)
When erythematous and inflamed, KP is referred to as keratosis pilaris rubra faciei (Fig. 7-8)
The condition is mostly of cosmetic significance
Clinical
Ammonium lactate (Lac-Hydrin), or other alpha- or beta-hydroxy acids, available in a cream or lotion, reduces roughness and softens the keratin plugs. It does not, however, lessen the redness caused by the condition
Urea-containing products, such as Carmol and Keralac, moisturize and soften dry, rough skin. They also help loosen and remove the dead skin cells
Gentle exfoliation twice per week with a loofah or a body scrub can help remove skin that has been softened by the urea or the alpha and beta hydroxy acid creams.
Topical retinoids may be an effective temporary treatment, but they can also cause bothersome skin irritations and exfoliation. Tretinoin (Retin-A Micro), tazarotene (Tazorac), adapalene (Differin), and trifarotene (Aklief) are examples of topical retinoids
Erythematous papulopustules (Fig. 7-9)
Unlike infantile and adolescent acne, there are no comedones and the course is self-limiting
Eruption is asymptomatic
Resolves spontaneously in weeks to months
Diagnosis is made clinically
A Giemsa stain may show yeast forms, neutrophils, and other inflammatory cells
When in doubt a Gram stain can rule out bacterial folliculitis, and a KOH fungal stain can rule out candidiasis
 Figure 7-9 Neonatal acne (neonatal cephalic pustulosis). Erythematous papulopustules on the cheeks resolved completely at 4 months of age in this infant. |
No treatment is required, as the condition self-resolves by 3 to 6 months of age
In severe cases, the application of a topical antiyeast imidazole such as ketoconazole 2% cream or econazole 1% cream twice daily can lead to improvement
Topical hydrocortisone 1% cream can be helpful if lesions are very red
Appears similar to typical acne vulgaris that is seen in adolescence with an admixture of acneiform papules, pustules, open and closed comedones, and cysts (Fig. 7-10)
Lesions are typically located on the cheeks, but can also be seen on the forehead, chin, and back
Cysts, draining sinuses, and deep nodules with potential for scarring occasionally occur
Onset is between 3 and 6 months and subsides at around 1 to 2 years of age commiserate with the normalization of androgen levels
Diagnosis is made clinically
First-line treatments are similar to those used for adolescent acne and include topical tretinoin 0.025% cream or benzoyl peroxide with, or without, a combined topical antibiotic such as Benzaclin (benzoyl peroxide 5% and clindamycin 1%)
In severe cases, oral antibiotics may be required
Antibiotic choices for acne at this age include erythromycin and trimethoprim/sulfamethoxazole
 Alert: Patients with infantile acne should have a complete physical examination with particular attention to other signs of androgen excess such as clitoromegaly, hirsutism, or pubic hair. If signs of androgen excess are present, referral to a pediatric endocrinologist is warranted.
Alert: Patients with infantile acne should have a complete physical examination with particular attention to other signs of androgen excess such as clitoromegaly, hirsutism, or pubic hair. If signs of androgen excess are present, referral to a pediatric endocrinologist is warranted. Figure 7-10 Infantile acne. In this 8-month-old boy there are acneiform papules, pustules, as well as open and closed comedones. |
Inflammatory lesions consist of papules, pustules (Fig. 7-11), and acne “cysts” (nodules)
Noninflammatory (comedonal acne) lesions appear as open comedones (“blackheads”) and closed comedones (“whiteheads”) (Fig. 7-12)
Mild acne consists of open and closed comedones and/or occasional papules and pustules
Treatment is often initiated with a topical retinoid alone (see Table 7.1) such as tretinoin, or in combination with a BPO agent or a topical antibiotic (see Table 7.2)
In addition, topical antibiotics alone or in combination with BPO such as Benzamycin, BenzaClin, and Duac gel may be prescribed (see Tables 7.3 and 7.4)
Azelex (azelaic acid cream 20% or gel 15%) can be useful to treat acne in pregnant women
Dapsone 5% or 7.5% gel (Aczone) is effective for inflammatory acne, particularly in adult females with acne
Topical minocycline 4% foam (Amzeeq) can be used to treat moderate to severe inflammatory acne in patients 9 years of age and older
Table 7.1 Topical Retinoids for Acne | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 7.2 Topical Combinations Containing Retinoids | ||||||||
|---|---|---|---|---|---|---|---|---|
|
Table 7.3 Topical Antibioticsa | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
Table 7.4 Combination Topical Antibiotic and Benzoyl Peroxide Agentsa | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


