Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
Autologous fat grafting is not a new technique. In the past many surgeons avoided its use because the results were poor and unpredictable. 1 , 2 However, in the 1980s, structural autologous fat grafting was developed, with well-defined indications, refined techniques, and predictable results. Fat grafting was introduced as a way to improve facial aesthetics. In recent years it has evolved into applications in more complex reconstructive procedures. Fat grafting can be used particularly on any facial area with a lack of soft tissue resulting from posttraumatic sequelae, following tumor resections, and as a refinement in craniofacial deformities. Its use has become widespread because it produces natural, long-lasting results with minimal donor site morbidity. 3 , 4
The complex field of orbitocranial and maxillofacial surgery includes long-term treatments. Fat grafting usually represents the last procedure in the reconstructive protocols.
The primary indications for fat grafting to the maxillofacial area are for restoration and rejuvenation of zygomas, periorbital region, cheeks, lips, nose, chin, jawline, and mandible. Recent applications include the correction of localized tissue atrophy, loss of substance resulting from trauma, tumor excision, and congenital complex craniofacial deformities, burns, and hemifacial atrophy (for example, from Parry–Romberg syndrome, scleroderma, and anophthalmic orbit). 5 , 6
Orthognathic surgery and fat grafting represent a new application and an appropriate indication. It is well known that this surgery moves the skeletal bases (maxilla, mandible, chin) but often this leads to a lack of soft tissue coverage. Some patients, particularly women, complain about this lack of soft tissue volume after surgery. Based on the so-called baby-face theory, increased volumes equal a youthful appearance. Fat grafting of the periorbital area, zygomatic area, the upper and lower marionette lines, and chin also improves skin texture and lightens the face.


This patient had a Class 3 dentofacial deformity malocclusion (A). After orthodontia, a high LeFort I (butterfly type) osteotomy and mandibular surgery (bilateral sagittal split osteotomy [BSSO]) were performed in one stage. Three years after surgery (B), the skeletal and soft tissue outcome is still stable, with high cheek bones and facial fullness, in this case without need for fat transfer. Another possibility is the insertion of cheek implants during surgery or as a secondary procedure. 7
Material and Methods
PREPARATION
Planning is always done with the collaboration of the patient, who must be fully informed of overall procedures.
For maxillofacial and craniofacial patients, the ideal position during surgery is supine. The head can be moved in different directions. Orotracheal intubation must allow movements of the tube, in particular when injection into the oral and perioral areas is being done. The surgeon must be able to evaluate the patient’s contours three-dimensionally throughout the procedure. Preoperative photos are displayed on the walls of the operating room or on a monitor.
MARKINGS
The preoperative plan includes a photographic setup according to Coleman’s guidelines. Different colored pencils are used on these photos in the areas to be injected, not injected, and, if necessary, areas from which excessive fatty tissue is to be removed. These markings are duplicated on the patient’s face before surgery.
ANESTHESIA
Patients receive a local anesthesia with lidocaine 0.5 % and epinephrine 1:200,000 and, if necessary, sedation or general anesthesia. For local anesthesia, calcium carbonate is added to reduce pain.
FAT HARVESTING, DONOR SITES, AND INCISIONS
Common donor sites are the periumbilical area, the abdomen, the lateral, anterior, and medial thigh, the “love handles,” and the knees. In children, buttock is an available source. Fat is taken from those areas through two or three small incisions (2 to 3 mm) that are large enough to permit insertion of the tip of the cannula.
The fat is aspirated using a 12-gauge Coleman aspiration cannula, usually 15 cm in length, attached to a 10 cc syringe. Cannulas for fat grafting must be atraumatic with a blunt tip to the grafted tissue during the harvesting and the placement as well. 8
FAT PROCESSING AND PURIFICATION
Fat processing and purification follows the classically described Coleman technique (see Chapter 1). We use centrifugation at 1300 rpm for 3 minutes. After centrifugation, only concentrated fat is used for injection. 9 , 10
TECHNIQUE
Coleman’s technique of fat grafting differs from other fat grafting techniques in both the harvesting and placement of the fat. The procedure is delicate. The harvested fat cells are gently centrifuged, resulting in a larger percentage of surviving tissue. Different kinds of cannulas have been used for harvesting and placement, keeping in mind the goal of minimal trauma to the adipocytes.
Coleman blunt cannulas with openings on either the convex or concave side allow excellent volume collection of fat parcels. By gently grasping the skin, the surgeon lifts away the subcutis from the underlying structures. Rapid movement of the syringe and needle in the subcutaneous plane allows atraumatic and bloodless collection of fat.
The cannula is inserted through small incisions made with a No. 11 blade or an 18-gauge needle. With linear deposition, the fat is layered into the area requiring enhancement, working from the underlying bone up to the skin surface. With each insertion, a very small quantity of fat is deposited as the cannula is withdrawn. The fat must be gently woven in several layers from the periosteum to the subdermis to optimize the potential for neovascularization, allowing the fat cells to survive and maintain the filamentous architecture. Some of the fat is slowly absorbed by the body, although the amount of resorption is unpredictable; the percentage varies from patient to patient but is usually from 20% to 30%. If a significant amount of fat is resorbed, a second or third procedure may be considered to improve the final result. In fact, using more fatty tissue in a single-step corrective procedure can cause poor vascularization and more resorption, particularly in areas covered by a thin layer of soft tissue, such as the maxillofacial area giving the so-called choke effect and the possible formation of cysts and fibrosis. In fat grafting, overcorrection, overgrafting, and the choke effect must be avoided. 11 – 12
Technical Pearls
• The perioral area cannot be treated with a regular cannula. A 20-gauge needle should be used to effectively reshape the perioral area, particularly the white roll. The lips should be treated in the same way when nonpermanent fillers, such as hyaluronic acid, are injected.
• When the philtrum is absent or poorly defined, resulting in a flattening and lengthening of the prolabium, it can be restored and revolumized by fat grafting in two parallel lines beside the nasal alae with a 20-gauge needle.
• In craniofacial deformities, one must bear in mind that the patient’s growth potential is always altered. Because of the high level of resorption, bone grafts should be performed a few times. The same situation applies to AFT. Resorption is higher. Fat grafting in patients with craniofacial deformities should be done as many as three to five times with a lapse of time from 6 to 12 months.
• Treacher Collins is a very complex syndrome to treat, because the SMAS and periosteum are missing. Even after repeated bony surgeries, the stigmata return, and the results might be unsatisfactory. There is a great amount of bony resorption, even after cranial bone grafting. Fat grafting improves the final result. 13
• In the anophthalmic socket, fat grafting provides an excellent solution to a volume deficiency. In the so-called postenucleation socket syndrome (PESS) there can be a lack of soft tissue, even after positioning an endoorbital implant. This can be improved by injecting the intraconal part as well as the upper sulcus on the upper eyelid.
• Recalcitrant ectropion (congenital, cicatricial, following trauma, or after various reconstructions) is challenging because of the resulting shortage of skin, muscles, and posterior lamellae. A palatal mucosal graft is useful for rebuilding the lamella, but it does not restore skin and the orbicularis oculi muscle. Lengthening of the lamella, combined in a second stage with very small parcels of processed fat, provides an effective solution to this problem and results in a lengthened lower eyelid with improved volumes and texture. 14 – 18

This patient underwent many different craniofacial reconstructive procedures, beginning at age 2, for the correction of a complex craniofacial malformation with hypertelorbitism (Tessier cleft 0-14). She was treated by Dr. Paul Tessier in Paris. The patient is seen at age 28 in preparation for a third fat grafting procedure. The face was marked with the operative plan, and fat grafting was then performed under general anesthesia.
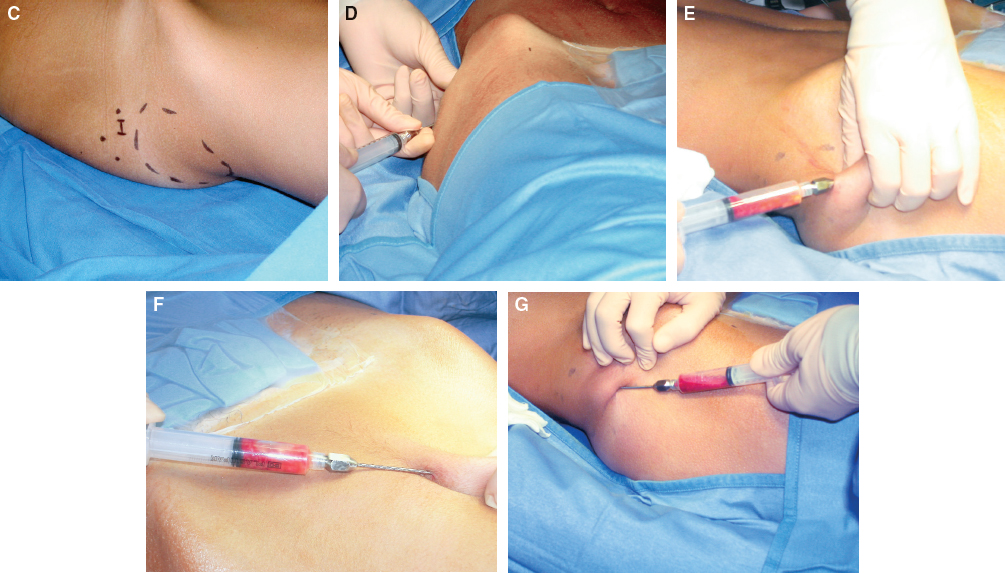
The donor sites were marked according to the classic Coleman protocol. Local infiltration was performed with 0.5% lidocaine with 1:200,000 epinephrine. Small incisions were made in the donor sites with 5.0 nylon or in pediatric patients using fibrin glue with Steri-Strips. Then blunt cannulas were inserted, and with a gentle negative pressure controlled with the hand, the fat was harvested from the periumbilical area, abdomen, thighs, and knees. After harvesting, donor areas should be massaged with a fibrinolytic ointment.

The surgeon should think three-dimensionally to assess volumes from all angles. In complex situations, the best position is to kneel, allowing a parallel view of the various facial contours.
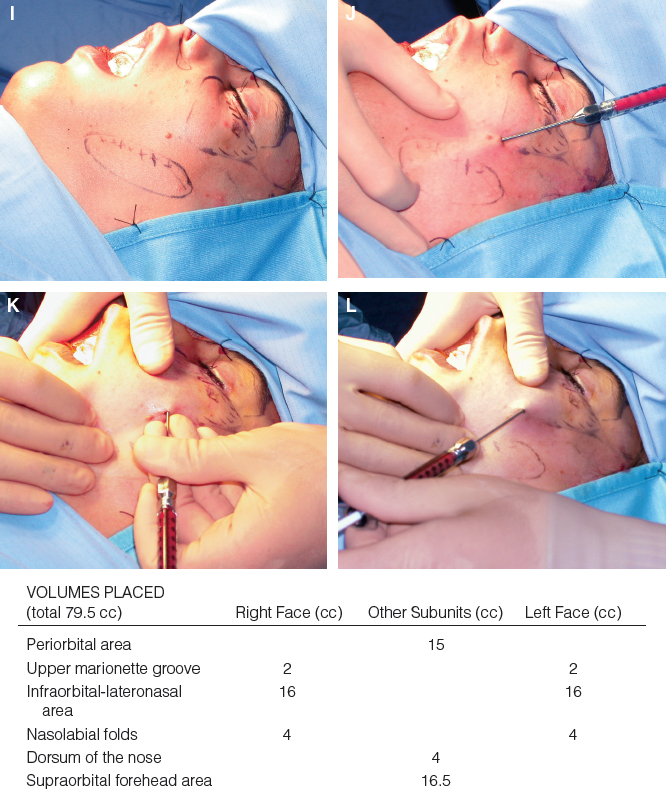
During each fat grafting session, the amounts of fat in cubic centimeters are recorded on a sketch of the face and reported on a table so that the surgeon can keep track of the fat injected in each area. This is useful for the following fat transplant stages.
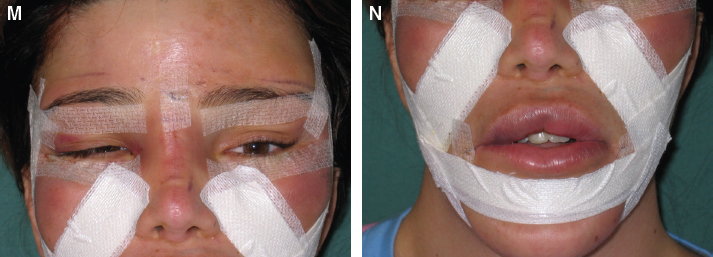
Strips of Microfoam tape are meticulously placed on the infiltrated areas and left in place for 5 to 7 days. This provides a protective barrier to reduce the formation of edema and prevents the patient from touching the skin. The patient cannot massage the infiltrated areas for approximately 3 weeks. In the postoperative period, the donor sites should be protected by a corset, and the use of antithrombotic socks is essential as in any other liposuction procedure.

The patient is shown at 2 years, at 17 years after total skeletal surgery, at 18 years after two fat grafting stages, and at 35 years after six fat grafting stages and 2 years after the last procedure. A total of 320 cc was transplanted over this period. Some procedures were also been performed on her nose and eyelids.
Related posts:
 Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
 Chapter 31 TREATMENT OF ROMBERG DISEASE
Chapter 31 TREATMENT OF ROMBERG DISEASE
 Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
 Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
 Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


