Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
The complex muscular activity of the velum and pharyngeal walls regulates speech resonance and permits speech articulation. Articulation is defined as the process by which speech is produced through coordinated movements of the soft palate, lips, and tongue, together with laryngeal sound emission. The levator veli palatini muscle lifts the velum in an upward and backward direction, whereas the palatopharyngeus and the pharyngeal constrictor muscles approximate the pharyngeal walls toward the midline. The lateral and posterior pharyngeal walls are pulled in and the passage between the nose and oropharynx gradually closes. To summarize, the concurrent action of the superior pharyngeal constrictor, levator veli palatini, and palatopharyngeus contribute to preventing air leakage from the mouth and pharynx into the nasal cavities. The site where separation between oropharynx and nasopharynx occurs is called the velopharyngeal (VP) port or sphincter. If various causative factors prevent proper closure of the port, air escapes from the oropharynx into the nasal cavity, altering the normal resonance balance and speech articulation. This condition is called velopharyngeal incompetence or insufficiency (VPI); it causes hypernasal speech, audible air turbulence, and articulation defects. Nasal regurgitation of food may occur during swallowing.
In an attempt to control VPI and to limit nasal air escape, several surgical techniques have been proposed, focusing either on the soft palate or on the posterior pharyngeal wall, or on both.
For musculature that has not been reapproximated during primary closure of the cleft palate or when scar tissue is present along the midline, impairing palatal elevation, Sommerlad et al 1 advocated soft palate re-repair. The double-opposing Z-plasty technique with creation of a levator muscular sling and simultaneous elongation of the velum was popularized in the United States by Furlow. 2 In 1946 Dorrance and Bransfield 3 described the pushback procedure to lengthen the soft palate by moving the entire palatal fibromucosa backward to minimize the existing space between the velum and the posterior pharyngeal wall.
Over the years, a group of surgical procedures, the so-called velopharyngoplasties, have been reported. Their common denominator was the reduction of the passage between the oropharynx and nasopharynx, either by interposing a mucosal flap outlined on the posterior pharyngeal wall and sutured to the velum, 4 – 7 or by creating a dynamic sphincter with the transposition of the two heads of the palatopharyngeus muscle to the midline and suturing them to the posterior pharyngeal wall. 8 Velopharyngoplasties are effective in diminishing the passage between the nasal cavity and the oropharynx, but they may have a relevant morbidity in the immediate postoperative period with severe pain and risk of bleeding, or in the long term with snoring and obstructive sleep apnea (OSA).
For moderate VPI, velopharyngoplasties are considered to be an overtreatment, whereas advancement of the posterior pharyngeal wall is one of the oldest solutions for VPI, beginning in 1878 with Passavant, 9 who proposed creating a mucosal ridge on the posterior pharyngeal wall to enhance the contact between the velum and the pharynx. Since then, a large variety of implants 10 – 12 or autologous tissue 13 , 14 have been positioned into the retropharyngeal space, with the aim of pushing the posterior wall of the pharynx forward and reducing the size of the nasopharyngeal port. To achieve a successful functional outcome, the implant or the autologous tissue must be located cranially in the pharynx at the point of the velar contact. However, over time, extrusion or dislocation of the implant in a caudal position has often been reported, making the prognosis for this technique questionable.
Recently, fat grafting to the velopharynx has proved successful in the treatment of VPI, and the regenerative properties of autologous fat are being widely studied. 13 – 16
Material and Methods
PATIENT SELECTION AND TREATMENT GOALS
Patient selection for fat grafting to treat persistent VPI is a critical step. Fat grafting can successfully correct only mild to moderate gaps of VP closure. Preoperative assessment is based on thorough evaluations performed by the surgeon, a well-trained phoniatrician, and a speech therapist.
The diagnostic assessment includes:
Perceptual evaluation, with spontaneous speech, repetition of sentences and phonemes to assess resonance, audible air escape and turbulence, articulation defects and dysphonia
Acoustic measurements, such as nasometry
Aerodynamic evaluation to calculate the nasal air leakage
Videofluoroscopy in multiple projections to estimate the size of the VP port
Videonasopharyngoscopy
In our clinical practice, perceptual evaluation, with video recording of speech samples and videonasopharyngoscopy, are the standard assessments for patient screening, whereas aerodynamic measurements are performed in selected cases and for research purposes. For evaluation of the results, the videos are blindly assessed by independent listeners with specific expertise in VP function. The results provide us with quantifiable data. It is of paramount importance to distinguish between VP insufficiency, related to anatomic defects that require surgical management, and VP dysfunction, associated with mislearning or neuromotor disorders, which can be primarily treated conservatively with speech therapy. Videonasopharyngoscopy is performed by introducing a flexible scope with a diameter smaller than 3 mm through the middle meatus. This procedure is also well tolerated by children. The data thus obtained inform the surgeon of the size and location of the VP closure gap. Videonasopharyngoscopy has been found to be superior to videofluoroscopy for identifying small VP defects and establishing their size, which is essential for surgical planning. 17
Depending on the considerations just described and on the nasopharyngeal gap closure, we rate patients according to a 5-point scale 13 : 0 = complete VP closure; 1 = an inconstant gap demonstrated by mucus bubbling; 2 = a gap involving less than 25% of the VP port at rest; 3 = a gap involving 25% to 50% of the VP port; 4 = a severe gap involving more than 50% of the VP port. Patients with gaps 1 to 3 (up to 50% of the VP port) are good candidates for VP fat injection, whereas patients with a number 4 gap are best suited for velopharyngoplasties, 6 – 8 because the augmentation resulting from fat grafting in in the four walls of the VP port would not be sufficient to reduce the size of the port and minimize the nasal air escape.
SURGICAL TECHNIQUE
The procedure is carried out under general anesthesia. Fat is usually harvested from the lower abdomen; however, in very slender patients, lipoaspirate is obtained from the inner knee or inner thigh. The area is infiltrated with 2.0% mepivacaine with a 1:100,000 epinephrine solution. A stab incision is made in the lower pole of the umbilicus with a No. 11 blade. A 2 mm three-hole disposable blunt cannula connected to a 10 cc Luer-Lok syringe is used. To provide negative pressure, the plunger of the syringe is retracted and is maintained in that position by means of a towel clamp. Once the necessary amount of fat is harvested, usually 16 to 20 cc, the incision is closed with a 5-0 nylon suture and an elastic garment is placed over the donor area to avoid possible hematoma formation. We routinely centrifuge the lipoaspirate at 3000 rpm. The fatty fraction of the lipoaspirate is transferred to a 3 cc Luer-Lok syringe for injection.
The patient is then positioned supine with a roll placed behind the shoulders to extend the neck. Endotracheal intubation is used. A Dingman mouth gag, suspended on a horizontal stand, facilitates exposure and depresses the tongue.
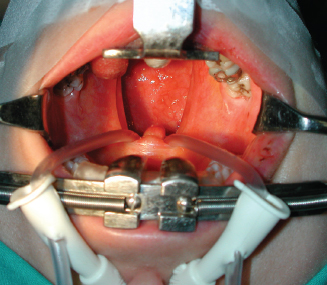
Placement is the critical step of the procedure and should be performed with utmost care. A Nelaton probe is inserted into each nostril, passed through the corresponding choana into the mouth, and the two heads of the probe are tied together so that the velum is gently retracted superiorly. The velum is then gently retracted to allow easy access to the nasopharynx where fat is to be placed. Fat grafting is performed to improve the contact between the velum and the posterior pharyngeal wall, which is clearly exposed.

To better visualize the nasopharynx and the soft palate and to make fat grafting as precise as possible, a 70-degree Storz 4 mm rigid nasal endoscope is connected to a videocamera and a monitor is used. A 3 cc Luer-Lok syringe is used for fat injection.
Injecting Fat Into the Posterior Pharyngeal Wall
Two stab incisions are made on the posterior pharyngeal wall at the level of the odontoid process, 5 mm lateral to the midline on both sides, with an 18-gauge needle or a No. 11 blade. In the past, we used a 19-gauge cannula for fat grafting, but often fat oozed out from the entry point. Currently we prefer to use a 21-gauge 60 mm long disposable, malleable microcannula (Thiebaud Medical, France), which is bent as needed. The entry point is through a very small incision to reduce the risk of fat leakage. The cannula is advanced in a cephalad and oblique direction, reaching the axis and then more laterally toward the ipsilateral pharyngeal wall in the submucosal plane. However, if excessive resistance is encountered while fat is being injected with the 3 cc syringe, a lipoinjection dosage handle (Medicon Instruments, Tüttlingen, Germany) facilitates the release of fat.
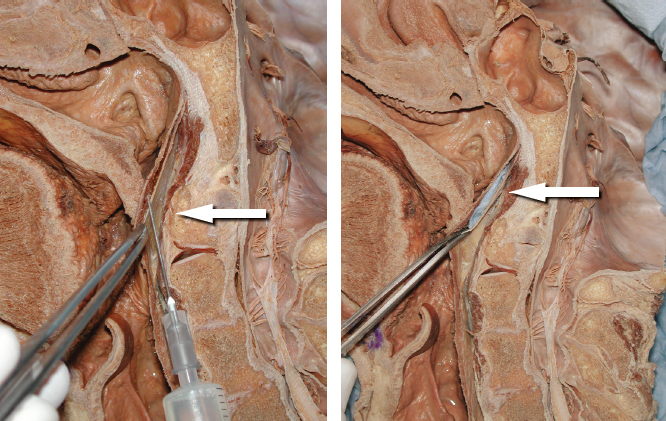
This cadaveric dissection shows the correct fat injection site into the nasopharynx at the level of the axis. Fat should injected in the submucosal plane (arrow) within the fibers of the superior constrictor muscle. On the right is a simulation of the grafted fat (shown in blue) (arrow).
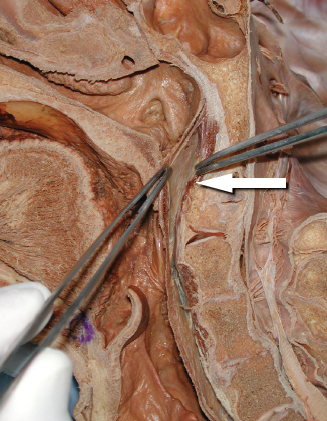
The level of infiltration is of paramount importance. Endoscopic assistance is critical to confirm assessment of the position of the cannula, the injection site, and the amount of fat released. The parcels of fatty tissue should be injected anterior to the prevertebral fascia, possibly within the fibers of the superior constrictor muscle at the level of the axis. However, injecting fat behind the prevertebral fascia, in the loose space that exists immediately anterior to the bodies of the vertebrae (as shown in the cadaveric dissection above), potentially results in dislocation of the graft caudally, along the natural cleavage plane. The dissection clearly shows this important detail. Numerous tunnels are made to maximize the contact between the grafted fat and the host tissue. Microfat parcels are released in multiple directions, always as the cannula is withdrawn, leaving a spaghetti-like thread of fat. 18
An average of 2 cc of fat is injected per side. The entry points are then closed with a 5-0 absorbable suture, if necessary. Injecting fat centrally along the posterior pharyngeal wall is not risky. However, as we shall see later, the risk increases when fat is injected laterally, where the large vessels of the neck course.
Related posts:
 Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
 Chapter 31 TREATMENT OF ROMBERG DISEASE
Chapter 31 TREATMENT OF ROMBERG DISEASE
 Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
 Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
 Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


