Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
A severe voice impairment has a detrimental impact on an individual’s quality of life and can have psychosocial and economic consequences. It may negatively influence social and professional relationships; the dysphonic person may even lose his or her job or can encounter career obstacles because of the inability to communicate properly and to convey his or her personality through voice features appropriate to the professional role. Vocal fold paralysis is a frequent cause of severe dysphonia, resulting from insufficient glottic closure; the air leak through the vocal folds not only causes a poorly audible, breathy voice, but also produces respiratory distress on phonation. Often patients exhibit significant phonatory effort and speech dyspnea, with consequent fatigue of the thoracic and neck muscles, and even dizziness caused by respiratory alkalosis. In cases of aphonia, patients become progressively exhausted by the effort required to sustain an audible voice.
Besides paralysis, several congenital or acquired defects of the vocal folds may significantly alter voice production because of inadequate vibration and contact of the vocal folds; in particular any scarring of the superficial layer can be the cause of a severe vibratory impairment. Voice rehabilitation is in most cases the initial treatment for glottic insufficiency, and can be effective in reducing dysphonia. 1 If voice therapy produces unsatisfactory results, surgical augmentation of the defective vocal fold can reestablish glottic competence. Glottic closure is necessary to ensure efficient vibration of the vocal folds and appropriate voice quality. The procedures used to correct glottic insufficiency include the medialization of the vocal fold using an external laterocervical approach 2 or augmentation by injecting the vocal fold with either an implant or autologous tissue. 3 The most commonly used implants and biomaterials are polydimethylsiloxane, 4 hydroxyapatite, 5 hyaluronic acid, 6 and micronized dermis. 7 The advantage of implants is the potential office treatment, under local anesthesia 8 ; however, local and systemic complications can occur, including foreign body reactions, extrusion, and reduced tissue pliability, with possible permanent worsening of dysphonia. 9
The autologous tissues utilized are mainly fascia 10 and fat. 11 – 13 The use of fat was introduced in the 1990s by Mikaelian et al 14 and Brandenburg et al, 15 who reported successful treatments for glottic incompetence. Subsequently, several authors published their experience but most of them noted that resorption occurred, causing failure over the long term. 16 – 18 Because of these unfavorable reports, vocal fold fat augmentation (VFFA) was considered a temporary correction of glottic incompetence for years, and most laryngologists preferred to use prosthetic implants 2 or injectable alloplastic materials, which obviated the need for a surgeon’s knife for harvesting and processing.
A new interest in the use of fat arose with the advent of the liposuction technique. In addition, basic research over the last decades has demonstrated that fat stromal vascular fraction contains a population of cells that have the typical features of mesenchymal stem cells (MSCs) 19 capable of self-renewal and differentiation into multiple cellular lineages. Several researchers around the world investigated the differentiation potential of the adipose-derived stem cells (ADSCs). 20 , 21 A characterization study was performed in our hospital on the lipoaspirate obtained from patients undergoing VFFA; the results have confirmed the high concentration of MSCs in the lipoaspirate and the embryonic state and multipotency of these cells. 22
Autologous fat obtained by liposuction is soft and easily diffuses into the vocal fold layers. It does not alter the elasticity of the glottic vibrator, even if injected in Reinke’s space, the superficial layer of the vocal fold. Chan and Titze 23 demonstrated that the viscosity of fat is similar to the content of Reinke’s space, so no impairment of vibration should be expected.
However, despite these favorable characteristics, the role of VFFA is still debated, mainly because of the unpredictability of the amount of resorption, possibly related to different modalities of fat harvesting and processing. Some authors reported good long-term results, 24 , 25 whereas other retrospective studies highlighted a high long-term failure rate. 17 , 18 Quantitative data about injected fat survival are still controversial. 26 , 27 Coleman 28 showed the importance of atraumatic fat harvesting, processing, and injection to preserve the integrity of the adipocytes and their fibrovascular support. We applied these principles while performing VFFA.
In this chapter, the authors will describe the technique utilized to improve voice quality and swallowing efficiency by means of VFFA in patients affected by defective vocal fold closure during phonation and swallowing.
Material and Methods
ANATOMIC AND PHYSIOLOGIC CONSIDERATIONS OF THE VOCAL FOLDS
The vocal folds are the source of the voice; sound is produced through vibration of the expiratory airstream. The larynx acts as an energy transducer capable of transforming aerodynamic power (from the expiratory airflow) into acoustic energy (the voice sound). Yet the vocal folds have a crucial role in other vital functions; they are a highly mobile and specialized structure with three main activities: respiratory, sphincteric, and phonatory. They open during inspiration to reduce resistance in the upper airway and to let the airstream flow toward the lungs, and they tightly close the airway passage during swallowing to prevent food from entering the airway. The respiratory and sphincteric activities of the larynx are essential for life and are the two primordial functions of this organ. Phonation is a more recent specialization of the vocal folds, essential for verbal communication and social relationships. The vocal folds close during phonation, thanks to contraction of the vocal fold adductor and tensor muscles. Complete vocal fold closure is a critical factor in achieving an efficient voice, because it allows subglottal pressure to rise up to a threshold that will elicit the folds’ vibration. A gap in closure gives rise to dysphonia; this can be caused by a motility impairment (more commonly a paralysis or paresis of the recurrent laryngeal nerve) or by a soft tissue defect of the vocal fold itself from congenital or acquired conditions. Laryngeal paralysis may be idiopathic, iatrogenic (mainly secondary to neck or thoracic surgery), or a consequence of accidental trauma. The majority of iatrogenic paralyses follow thyroid ablative surgery. A vocal fold tissue defect may be caused by previous endolaryngeal surgery for benign or malignant lesions or may result from minor malformations. 29 Less frequently, vocal fold scarring is caused by external trauma (laryngeal fracture) or prolonged endotracheal intubation.
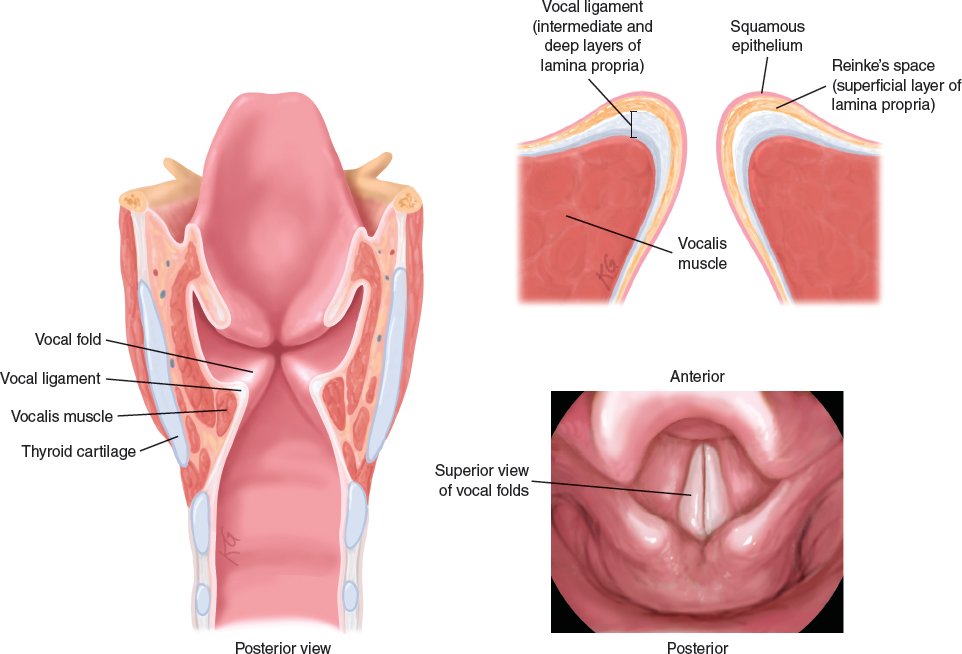
Understanding the phonatory deficits caused by laryngeal paralysis requires knowledge of the vocal fold’s anatomy and physiology. The above drawings show a posterior view of the larynx and a vocal fold. The complex structure of the vocal folds is illustrated, with a detailed view of the vocalis muscle. The vocal fold comprises several layers. The innermost part is the vocalis muscle, which extends from the arytenoid to the inner angle of the thyroid cartilage. On its surface lies the lamina propria, which is composed of three layers: superficial (rich in elastin fibers and fluids, called Reinke’s space), intermediate, and deep (these last two, rich in collagen fibers, constitute the vocal ligament). The outermost layer is a stratified squamous epithelium. These components have different viscoelastic properties and play different roles in sound production. Schematically, they form a body (the intermediate and deep layers of the lamina propria and muscle) and a cover (epithelium with the superficial layer of the lamina propria).
The body-cover model helps explain how sound production takes place: a mucosal wave is generated by the air pressure in the lower part of the vocal folds and flows upward, giving rise to the vibratory cycle with repeated opening and closing of the folds.
The body of the vocal fold acts as a stiff inner component that allows the overlying flow of the mucosal wave generated into the pliable cover. It can be easily understood that a voice alteration may be caused either by weak or defective closure of the vocal folds or by stiffness of the superficial layer, which plays a key role in sound production.
If vocal fold closure is inadequate, the sphincteric function of the larynx can be affected, and aspiration of food can occasionally occur, particularly foods with a liquid consistency. Hence patients affected by severe dysphonia caused by glottic incompetence often report episodes of coughing while ingesting fluids, resulting from episodes of leakage in the supraglottis or aspiration below the vocal folds.
Fat grafting in the vocal folds fulfills one or both of the following goals:
Medialization of the defective fold to obtain complete closure during both phonation and sphincteric closure of the larynx (for example, swallowing, coughing, and the Valsalva maneuver)
Restoration of the defective gliding tissue in the superficial layer (cover) to reestablish floating of the mucosal wave and sound production.
INDICATIONS AND CONTRAINDICATIONS FOR VOCAL FOLD FAT AUGMENTATION
In our experience, the main indication for VFFA is insufficient closure of the vocal folds as a result of the following conditions:
Unilateral laryngeal paralysis or paresis (caused by a lesion of the inferior laryngeal nerve, also known as the recurrent nerve), which causes a flaccid paralysis of the unilateral vocal fold
Malformations of the vocal fold structure, such as sulcus glottidis or sulcus vergeture (congenital adherence of the epithelium to the ligament, with missing gliding tissue of Reinke’s space)
Scarring from previous surgery (for benign or malignant lesions of the vocal folds)
Scarring from prolonged intubation or laryngeal fracture or contusion
Soft tissue defects from previous oncologic surgery
Vocal fold stiffness from previous radiotherapy
Aging-related laxity of the vocal muscles, (this condition is known as presbyphonia)
A secondary procedure following failure of a previous augmentation by injection of an implant (with an eventual inflammatory reaction and secondary tissue stiffness)
All the conditions mentioned have been encountered and treated in our practice.
The following contraindications have been identified:
Recipient site: The procedure is absolutely contraindicated if the patient is affected by effort dyspnea caused by glottic stenosis. The typical case is paralysis of both vocal folds.
Donor site: No contraindications are known; the procedure can be easily performed, even in underweight patients, because the amount of fat necessary to achieve VFFA is very limited.
PREOPERATIVE EVALUATION
Laryngeal Assessment and Voice Evaluation
A multidimensional assessment is essential for evaluating voice outcomes. It is important to highlight not only the “aesthetic” acoustic changes of voice quality but also to demonstrate whether the fatigue determined by voice production has been reduced. Therefore the patients undergo the following evaluations preoperatively and postoperatively:
Videolaryngostroboscopy using a flexible or 70-degree rigid fiberoptic endoscope, which allows the preoperative documentation of the site and severity of the glottic gap, vocal fold vibration abnormalities, and objective assessment of postoperative changes
Maximal phonation time measurements obtained during the production of a sustained vowel /a/. This is considered the simplest way to obtain an indirect measure of glottic closure. This is an aerodynamic parameter, which is also influenced by the patient’s vital capacity.
Perceptual voice evaluation by means of the GRBAS, 30 which includes these five parameters:
Grade of dysphonia (G)
Roughness (R)
Breathiness (B)
Asthenia (A)
Strain (S)
Patient self-assessment by means of the questionnaire Voice Handicap Index (VHI). 31
Acoustic analysis of a voice sample by the MDVP software (Kay Pentax).
Measurement of aerodynamic parameters such as oral airflow during phonation and subglottic pressure.
In selected cases, radiologic studies (MRI and/or CT scan) have been obtained either postoperatively or both preoperatively and postoperatively to evaluate persistence of the fat graft within the treated vocal fold.
Related posts:
 Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
 Chapter 31 TREATMENT OF ROMBERG DISEASE
Chapter 31 TREATMENT OF ROMBERG DISEASE
 Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
 Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
 Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


