Chapter 31 TREATMENT OF ROMBERG DISEASE
Romberg disease (RD), also called Parry–Romberg syndrome, is a rare, acquired disorder characterized by progressive hemifacial atrophy of the skin and soft tissue. Some cases result in atrophy of muscles, cartilage, and the underlying bony structures. The cause is still unclear. Several theories have been posited for its pathogenesis:
Infection
Sympathetic nerve dysfunction
Trigeminal nerve involvement
Autoimmunity, including scleroderma
Trauma
Heredity
Neurocutaneous syndromes
Abnormalities of neural tube crest cell migration
Cranial vascular malformation
Disturbance of fat metabolism
Endocrine disturbances
The occasional RD cases are familial and point to a genetic predisposition. Some authors have suggested the mode of inheritance to be autosomal dominant with incomplete penetrance. According to a survey of nearly 100 of our RD patients, most of their mothers did not have any abnormal events during their pregnancy, and their brothers or sisters were also healthy, whereas nearly half of the RD patients had a history of trauma. The clinical signs of RD include neurologic, ophthalmologic, cardiac, rheumatologic, infectious, endocrine, maxillofacial, and orthodontic manifestations as well as autoimmune diseases, congenital diseases, and pregnancy. 1
The traditional treatment of hemifacial atrophy was free fat grafting, such as the following:
Dermal fat or aponeurosis fat transplantation: This technique is suitable for mild and moderate localized atrophic areas but cannot be used in large areas. Moreover, the operation must be done stage by stage on different operative sites, with an interval between procedures of at least 6 months. The absorption rate of the dermal fat is 20% to 40%.
Microvascular anastomosis tissue transplantation, involving larger omentum transplantation, muscle transplantation, or fat and aponeurosis flap transplantation. The latter two methods avoid the potential complications associated with entering the abdominal cavity.
Although these methods can ameliorate facial asymmetry, 2 – 7 there will be obvious donor site scars, that may lead to deformity or dysfunction. The recipient areas always result in a bulky appearance, leading to an unnatural expression. One or more operations are required to thin the bulky flap. In addition, the skin from another part of the body is not likely to match the color of the facial skin, and scars will be evident. The procedures require hospitalization, with multiple procedures under general anesthesia, which costs more. Patients have been dissatisfied with the results of all of these approaches.
Alloplastic materials first came into use in plastic surgery during the 1960s and 1970s. 8 , 9 Historically, many prosthetic materials have been used to treat hemifacial atrophy, including silicone rubber, expanded Teflon, polytetrafluoroethylene (PTFE), and others. All of these materials cause an unnatural sensation in the filled area, and they may become displaced, revealing the presence of the prosthesis. Heterologous soft tissue filler such as collagen was reported to produce good results, 10 but these lasted for only a very short period of time; other authors indicated that collagen also might depress the body’s immune mechanisms. Acellular dermal matrix has a high resorption rate and often triggers allergic responses.
Flaps and alloplastic materials have been used to treat the atrophy of RD patients traditionally, but fat grafting has become more popular and provides more satisfactory results. With fat transfer, the contours of face as well as the texture of skin are improved, a natural facial expression is restored, and no scars or donor site issues are involved.
Pathophysiology of Romberg Disease
Pensler et al 11 reported that 85% of RD patients have atrophy of both soft tissue and bone. If atrophy began after the individual was more than 10 years of age, when his or her facial bones had developed almost completely, only the soft tissue of the face would be affected. However, if the condition began before 10 years of age, the atrophy would lead to facial malformation and a distorted appearance. Histopathologic examination of affected RD skin usually reveals atrophy of the epidermis, dermis, subcutaneous tissue, skin adnexa, vessels, and hair follicles, as well as skin fibrosis with collagen fiber thickening and skin edema. Some patients show bandlike alopecia, homolateral segmental vitiligo, hyperpigmentation, morphea, and linear scleroderma en coup de sabre.
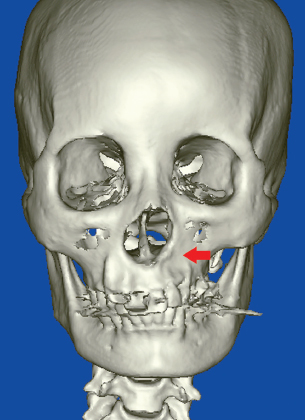
This three-dimensional CT construction shows the bone atrophy in the left side of the face in an RD patient.

Patients are sometimes diagnosed as having localized scleroderma. This patient has scleroderma en coup de sabre. Actually, distinguishing RD from localized scleroderma is very difficult. These conditions have a similar age of onset and present as lesions that progress over time until they stabilize a few years later. They have been found to coexist in many patients. Both may respond to immunosuppressive treatment.
Material and Methods
CLINICAL EVALUATION
Because there has been no uniform classification standard for RD, we have instituted the following method that divides patients into three groups: slight, moderate, and severe atrophy. Depending on the atrophic depth, the scores are as follows:
Involving skin or subcutaneous: 1 point
Involving muscle: 2 points
Involving mucosa: 3 points
Involving bone, cartilage, or teeth: 4 points
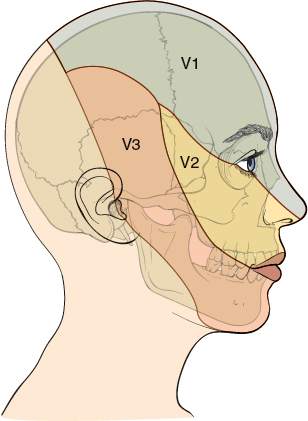
Then, depending on the area of atrophy, the face can be divided into upper, middle, and lower parts, just as in the three branches of the trigeminal nerve: the ophthalmic nerve, maxillary nerve, and mandibular nerve distribution areas. The scores are as follows:
Involving one area: 1 point
Involving two areas: 2 points
Involving three areas: 3 points
Then we summarize the two scores:
Slight atrophy: 2 or 3 points
Moderate atrophy: 4 or 5 points
Severe atrophy: 6 or 7 points
SELECTED OPTIONS FOR RECONSTRUCTION
Patients with slight atrophy and some with moderate atrophy can be successfully treated with fat grafting only. Those with severe or partial moderate atrophy may have involvement of hair, eyebrows, or teeth, which cannot be corrected with fat grafting. For severely affected patients with alopecia, we recommend reconstruction with a soft tissue expander. The expander can be embedded under the scalp during the same procedure in which fat grafting is performed. After 3 to 6 months of tissue expansion, the second fat grafting procedure can be done and the tissue expander removed as the alopecia is repaired. Patients with sparse eyebrows will have sunken arcus superciliaris (the supraorbital margin); these individuals will require hair transplantation 3 to 6 months after fat grafting, when the surviving fat can provide a more robust blood supply and nutrition to the hair follicles. The soft fat will provide better “soil” than atrophic skin attached to bone for “seeds” (hair follicles) to be implanted. 12 For male patients, if the eyebrow on the unaffected side is very full and bushy, a free scalp transplantation to replace the alopecic eyebrow will be a better choice for reconstructing a new eyebrow.
An atrophic defect of the nasal ala is challenging to correct. Only rarely can an atrophic ala be enlarged and recontoured with fat grafting. In most patients, auricular composite tissue may need to be transferred to the atrophied ala, or a part of the unaffected ala can be transplanted. If the patient does not want a permanent effect or any scarring, he or she can choose to have the deficient ala injected with hyaluronic acid (HA). Some patients may not want a scar on their forehead area (as might occur from the use of a tissue expander to provide tissue for nasal reconstruction) or a defect of the ear from cartilage harvest. A few RD patients may also develop a malocclusion, in which case orthognathic surgery can be performed before fat grafting is undertaken.
It is important to ensure that the patient is within his or her stable phase. According to a number of published reports, Parry–Romberg syndrome slowly progresses over 2 to 20 years before stabilizing. 13 – 21 The stable phase should be longer than 2 years; otherwise the fat graft may atrophy along with the surrounding tissue. In patients with severe defects who have correctable skeletal abnormalities, skeletal contour surgery should be completed before correction of soft tissue with fat grafting. When the subcutaneous tissue is almost completely atrophic, earlier intervention can improve or prevent further atrophy of the overlying skin and may prevent or lessen subsequent skeletal wasting.
Every RD patient should be well informed about fat grafting as an option for treatment of hemifacial atrophy, including its potential benefits, limitations, and complications. Maximal efforts during preoperative teaching are made to ensure postoperative compliance. Patients must understand that they could require two or three sessions of fat grafting with intervals of 3 to 6 months between procedures. If fat grafting is performed during a patient’s stable phase, there is no evidence that he or she will redevelop atrophy. Most patients will remain stable after adolescence. Careful examination during the preoperative visit is essential to confirm the extent and thickness of facial recontouring required and to determine the quantity of fat grafts needed. Standard preoperative photos, Visia scans, and three-dimensional scans are taken of each patient. The images can be used to discuss the extent of the procedure and the expected results.
Related posts:
 Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
Chapter 30 STRUCTURAL FAT GRAFTING IN CRANIOFACIAL SURGERY
 Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
Chapter 35 VOCAL FOLD AUGMENTATION IN THE DYSPHONIC PATIENT
 Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
Chapter 34 TREATMENT OF VELOPHARYNGEAL INCOMPETENCE WITH AUTOLOGOUS FAT GRAFTING
 Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
Chapter 33 FAT GRAFTING IN HIV-POSITIVE PATIENTS
 Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
Chapter 32 FAT GRAFTING IN ORBITOCRANIAL AND MAXILLOFACIAL RESTORATION: FROM SURGERY TO REGENERATION
 Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Chapter 25 STRUCTURAL FAT GRAFTING IN THE NOSE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


