Case 40 Gynecomastia
40.1 Description
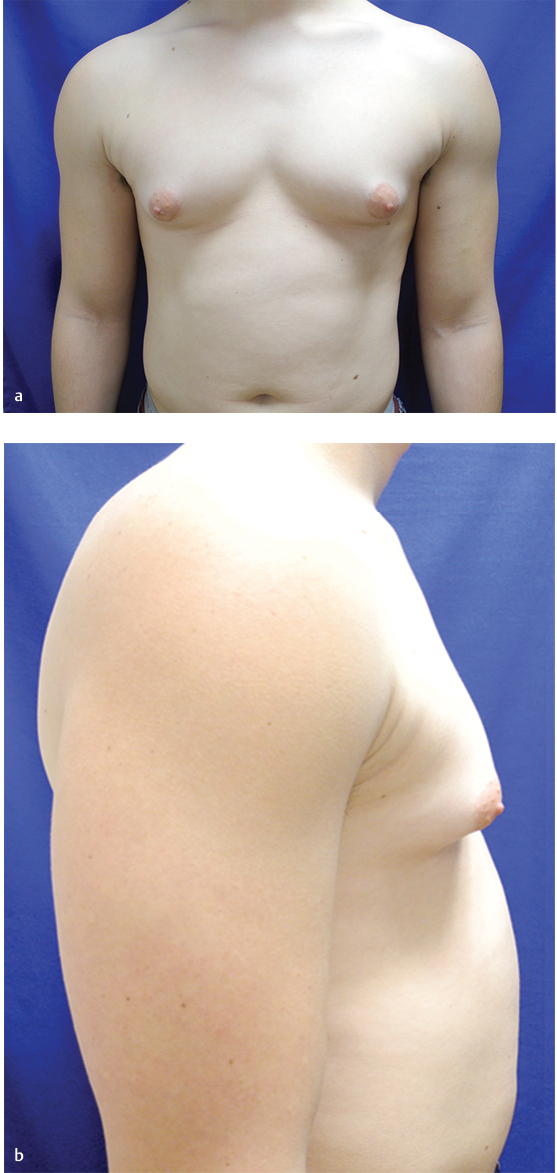
Adult male with bilaterally symmetric, mildly enlarged breasts
Minimal excess skin
Protuberance of nipple-areola complexes (NACs)
Normal body habitus, without evidence of obesity
40.2 Work-Up
40.2.1 History
Onset of breast development
Changes to breasts over time
Presence of breast pain, breast enlargement, and nipple discharge
Recent weight changes
Personal history of diseases of the liver, adrenal glands, thyroid, or kidneys, HIV, and complete medical history; family history of breast cancer
Current and prior medications or drug use
Certain medications have been associated with gynecomastia (see Table 40.1)
40.2.2 Physical Examination
Breast examination
Identify if breast enlargement is due to fat or glandular hypertrophy
Pseudogynecomastia: Bilateral breast enlargement due to fat deposition without an increase in glandular tissue
Finding concerning for malignancy: Small, firm, eccentricity, chest wall fixation, nipple discharge, and skin dimpling
Tenderness: >70% of benign gynecomastia will have tenderness
Presence of dense fibrous tissue
Degree of skin excess, breast ptosis
Simon’s classification, based on degree of tissue and skin excess
Type I: Minor enlargement of breast without skin excess
Type II: Moderate enlargement of breast
Type IIA: Without skin excess
Type IIB: With minor skin excess
Type III: Breast enlargement with skin excess
Virilization: Feminizing characteristics, lack of normal male hair distribution, voice changes
Testicular examination
Thyroid examination
Abdominal examination
Evaluate for organomegaly, abdominal masses, and ascites
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


