Case 28 Gender Transition (Male-to-Female)

28.1 Description
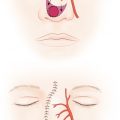
Some breast development noted, well-defined lateral pectoral border, no significant volume discrepancy, laterally positioned nipple-areolar complexes (NACs), and pink scars overlying sternum and left shoulder
Tuberous breast deformity with herniation of breast tissue into the NAC, constricted base, and deficient lower pole
28.2 Work-Up
28.2.1 History
Duration of social transition as female
Use and duration of feminizing hormone therapy and stability of breast development
Use of padded brassiere or volume-enhancing prosthetic
History of hypertrophic scarring or keloids
Weight stability
Medical comorbidities
Psychiatric history and any established relationship with a mental health professional
History of smoking
Family history or personal history of breast cancer
28.2.2 Physical Examination
Volume of native breast tissue
Breast measurements: Sternal notch to nipple distance, inframammary fold (IMF) toNAC distance, breast width, height, projection, soft tissue pinch, and NAC dimensions
Skin quality
Grade of breast ptosis
Masses, discharge, or lymphadenopathy
Chest wall contour
Skin rashes
28.2.3 Pertinent Imaging or Diagnostic Studies
Breast imaging if any abnormality is noticed on examination
28.3 Consultations
Mental health professional:Should be involved throughout the preoperative and postoperative process
Endocrinologist or primary physician:Coordinating hormone therapy and follow-up
28.4 Patient Counseling
Effects of feminization hormone therapy on the chest
Mammogenesis (similar to pubertal development) to varying degrees
Inherent differences between the male and female chest relevant to top surgery
Male chest is wider with more pectoral muscle development and stronger pectoral fascia
Male areolae are smaller and more laterally positioned
The male chest has a shorter distance between nipple and inframammary crease
Goals of surgery: Achieve a more feminine profile, cleavage, and desired breast volume
Smoking cessation encouraged
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


