Case 24 Aging Upper Face

24.1 Description
Fitzpatrick I skin type
Lateral brow ptosis with tattooed brows above supraorbital rim
Dermatochalasis of the upper eyelids; pseudoherniation of lower eyelid fat pads
Midface descent with a prominent arcus marginalis/infraorbital rim
24.2 Work-Up
24.2.1 History
Identify medical conditions that may increase the risk of complications
Blepharochalasis, Graves’ disease, glaucoma
Previous periorbital and facial procedures
Recent laser-assisted in-situ keratomileusis (LASIK) or cataract surgery: Should not undergo blepharoplasty for at least 6 months following procedure
History of dry eyes/seasonal allergies
Hormone replacement therapy: 70% higher risk of dry eye
24.2.2 Physical Examination (Analysis of the Upper Third of the Face)
Forehead analysis: Hairline (brow height), transverse and glabellarr hytids
Eyebrow analysis: “Ideal brow”
Location: Relation between hair-bearing brow and supraorbital rim
Peak: Should be located at or just lateral to the lateral limbus
Evaluate for brow ptosis and compensation
Upper eyelid analysis
Upper eyelid/Iris relationship: Covers 2–3 mm of superior limbus
Upper eyelid crease: Female (7–10 mm), male (6–8 mm), Asians (variable but low)
Lateral extension of the eyelid crease onto the lateral portion of the periorbital region is a marker of forehead ptosis (Connell’s sign)
Lower eyelid analysis
Lower eyelid/Iris relationship: Minimal to no scleral show, ideally covers 0.5 mm of the lower limbus
Tear trough deformity
Malar support
Positive vector
Negative vector— relative scarcity of skin, hemi exophthalmos
Ocular examination (Table 24-1)
Eyelid ptosis
Patient focuses on a light source with both eyes
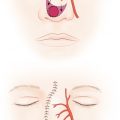
Margin reflex distance (MRD1): The distance from the pupillary light reflex to the upper eyelid margin (Fig. 24-1)
Normal MRD1: 4–4.5 mm
Levator excursion
Hold brow in resting position. Ask patient to look up and measure excursion of the upper eyelid with a ruler (normal >10 mm)
Dermatochalasis: Visual field test to document
Visual acuity
Dry eyes: Schirmer’s test, Bell’s phenomenon (see Chapter 25)
Ectropion/lower eyelid laxity
Lower eyelid distraction <7mm, lower eyelid snap test
MRD2: Measure the distance from the pupillary light reflex to the lower eyelid margin (Fig. 24-2)
Normal MRD2: 5–5.5 mm
Table 24.1 Ptosis classification
Ptosis
Mild
Moderate
Severe
MRD1
2–2.5 mm
1–1.5 mm
<1 mm
Levator Excursion
Good
>10 mm
Fair
5–10 mm
Poor
<5 mm
Abbreviation: MRD, margin reflex distance.


Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


