Case 14 Congenital Facial Paralysis

14.1 Description
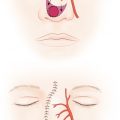
Complete left-sided, unilateral facial nerve palsy
Inferior descent of left oral commissure
Inability to completely close left eye with intact Bell’s reflex
Left sclera white, without injection/irritation
14.2 Work-Up
14.2.1 History
Family history of congenital palsy
History of birth trauma
Symptoms of dry or irritated eyes
Feeding problems or speech difficulties
Lack of lateral eye movement (Moebius syndrome)
14.2.2 Physical Examination
Observe facial movement during conversation/build rapport with patient
Sequentially test facial nerve function of all branches on both sides
Test for Bell’s reflex: Hold eyelid open as patient actively tries to close eye
This is a protective phenomenon
Inspect sclera for signs of irritation/dryness
Look for lower eyelid malposition
Donor nerves: Test for contralateral buccal branches of facial nerve (smile), ipsilateral nerve to masseter (bite), spinal accessory nerve (shoulder shrug), and hypoglossal nerve (tongue movement)
14.2.3 Diagnostic Studies
Obtain computed tomography (CT) scan, only if there is concern for concomitant craniofacial microsomia
14.2.4 Consultation
Best managed by a multidisciplinary team: Plastic surgery, pediatric otolaryngology, neurosurgery, pediatrics, speech pathology, child psychology, nutrition, social work, and nursing.
14.3 Patient Counseling
Emphasize the need to maintain corneal lubrication to prevent desiccation and ulceration.
Discuss the pros and cons of single-stage surgery (nerve to masseter) and two-stage surgery (cross-facial nerve graft).
Discuss the timeline of two-stage facial reanimation beginning with cross-facial nerve graft after age 4, followed 6 months later by gracilis free flap.
Explain the additional time needed (6–12 months) for movement to begin.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


